So what did they do? They took a group of lab rats and made them obese with trans fatty acid enriched Crisco as 60% of their calories. They then split the rats in to two groups, one was given 60% of calories as carbohydrate through out. The other group was given 5% carbohydrate for 2 weeks then 15% carbohydrate for a month, à la Atkins. Both groups were moderately energy restricted, dictated by a somewhat random decision protocol.
There was a parallel group eating crapinabag (CIAB) throughout (no Crisco). Glucose tolerance tests, with insulin measured at 20 minutes, were performed at various time points.
What went wrong in 2006?
Things started well with the Crisco rats having higher blood glucose at 10 minutes in to the GTT than the CIAB rats. Insulin levels were a lot higher in the Criso rats 20 minutes in to the test by which time glucose was identical between Crisco and CIAB groups. That's Graph A. Crisco causes insulin resistance.

Things were going reasonably well for Atkins bashing at the end of the two week "Atkins Induction" phase. During GTT the 60% carb group were slightly lower in glucose and this made p<0.05 at 10 minutes. However the cracks are beginning to show. The "Atkins Induction" group had an insulin at 20 minutes in to GTT of 600pM, the 60% carb group needed an insulin of over 900pM to achieve the marginally lower glucose level at this point. The insulin values were, luckily for A&A, not significantly different. Fasting insulin at this point was also lower in the "Atkins Induction" group. A&A were lucky on the p values here too. Here's graph B with that spiked glucose at 10 minutes:
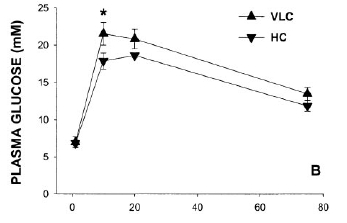
By the end of the experiment at 14 weeks the Atkins Group had been given more (15% of calories) carbohydrate. The GTT at this time point is shown here:

Now you need to get your glasses on for this one. Can you see any difference between the "Atkins Ongoing Weight Loss" (VLC) group and the 60% carbohydrate (HC) weight loss groups? No? Me neither.
Insulin values were slightly better in the 60% carb group but again nothing significant. Both weight loss groups had lower insulin values than the CIAB group! All NS again.
So there we have it: Atkins Ongoing Weight Loss, as interpreted by A&A, gives a GTT curve which is superimposed on the 60% carbohydrate weight loss group. ATKINS is GOOD!
There is a load of bollocks in the discussion about the impaired insulin response in the Atkins group in graph B. To me shifting glucose with a lower insulin level is good, not bad. The spike at 10 minutes is the only saving grace to the funding generating ability of this study.
But graph C is just hysterical.
Okay, A&A are not stupid. They worked out exactly what went wrong in graph C and what was going well in graph B.
So they went out and got more funding to demonstrate CONCLUSIVELY that the Atkins Diet makes you diabetic. They got that funding. These people are good, make no mistake. They got the desired result second time round. How many people get a second chance like this? They published in 2010.
Here is graph a from 2010, directly comparable to graph A from 2006.

Very similar but tidied up in 4 years of refining the model. Or maybe the CIAB has been improved. Anyhoo, same result. Crisco does nasty things to GTT curves.
Next is graph b, which is like graph B above but is after a month rather than 2 weeks and has the on going Crisco group included. The very low carbohydrate group is looking a lot like the Crisco group by now...

But here is the Money Shot in graph c from 2010. Just look at the Crisco curve (HF) and the 5% carbohydrate (VLC) curve. Just look at that fit!

I told you these people were good!
But also go back and look at the blooper graph C from 2006.
So what is going on?
There is a nice pointer in line seven of Table 2, "Soleus TAG". This is the amount of intra myocyte lipid in a typical muscle. It is a marker of how reluctant that muscle is going to be to accept glucose. Two groups have high soleus TAG. The Crisco poisoned (HF) group throughout and the VLC group at 16 weeks.

The explanations for why these two groups have high soleus TAG is likely to be different. Both will, in all certainty, reflect elevated FFAs in the plasma. But the Crisco poisoned group will have elevated FFAs, 24/7, despite 15% of calories as starch. We know from the 2006 blooper that 15% of calories as starch will give a GTT curve in VLC rats which matches the 60% carb group EXACTLY. Not so if you are Crisco poisoned.
The VLC rats on 5% of carbs will have elevated FFAs 24/7 because they would be dead without them. They are on a starvation diet of which only 5% is carbs. Without FFAs they would run their muscles on glucose. They don't get enough glucose per day to do this and still keep their brain alive. Death is not an option.
So the Crisco group has elevated TAG in soleus muscle in the presence of carbohydrate in the diet. It's pathological. The VLC group has elevated TAG in their soleus muscle because they had minimal free glucose available, which is physiological.
BTW either fasting or a brief period without carbohydrate will promptly elevate muscle TAG in humans. It is an utterly normal response to a reduced supply of glucose. The actual signal for muscle insulin resistance is not likley to be the tri acyl glycerol molecules themselves because athletes have bucket loads of this without insulin resistance. More likely is a more ephermeral moiety such as Acyl-CoA molecules or diglycerides which more closely reflect FFA supply. In a GTT the glucose supply is massively supraphysiological. For insulin sensitivity to return to LC muscles it takes time for insulin to spike, insulin to get to adipocytes, adipocytes to respond to insulin, FFA level in blood to drop and FFA derivative level in muscle to drop. It's hardly surprising that the 10 minute glucose peak was higher in the VLC rats during GTT. However, as soon as the muscles clear FFA derivatives they are still geared up to go with glucose, nae problem, nae bother. I'll come on to issues with insulin later. Obviously the Crisco poisoned rats are obese and their adipocytes will have an inability to suppress FFA release in response to insulin. That's how it is if you eat Crisco.
Let's look at the insulin responses. All of the fasting insulin levels were about the same. Obviously the VLC had the lowest insulin and almost certainly the lowest HOMA score although p might still have been > 0.05. By week 16 the insulin response to GTT was interesting.
The VLC rats mimicked the Crisco (HF) group's glucose curve. But they did it with just 1.79ng/ml of insulin. The Crisco rats needed 2.93ng/ml of insulin (p<0.05). The lower curve with open diamonds is the 60% carb group. The curve looks good until you realise that these rats needed as much insulin as the Crisco rats to achieve this beautiful curve, nearly twice that in the VLC group (2.95ng/ml vs 1.79ng/ml, p<0.05).
So which rats are the most insulin sensitive? Not the Crisco rats. I'll accept that. Just say no to Crisco... It is completely arguable between the VCL and 60% carb group.
BUT. What would have happened if the VLC group had produced the same insulin response as the 60% carb group? Impossible, scream Axen and Axen. The VCL group have a blunted insulin response. It makes them well on the road to diabetes, metabolic syndrome, blindness, dialysis, we need the funding...
Calm down Peter, bit OTT there!
Except metabolic syndrome is characterised by elevated insulin, not depressed insulin. Duh.
I have to thank Helen who placed a comment on another post. She pointed out that glucokinase in the pancreas, the enzyme which the pancreas uses to sense glucose in the portal blood, is down regulated in response to carbohydrate restriction. Oh.
It is, err, up regulated in carbohydrate surplus.
This is what "bit" Axen and Axen in 2006. It looks like 15% of calories as carbohydrate in a VLC non-Crisco situation is adequate (on a high protein background) to allow pancreatic insulin secretion in response to glucose to become identical to that produced by rats on a 60% carbohydrate diet. Muscle TAG and associated molecules will drop too. Hence the overlay of the GTT curves in 2006.
Let us assume, very reasonably, that the VLC rats in 2010, on a 5% carb, energy restricted diet, are not expecting to deal with hyperglycaemia any time soon. They down regulate glucokinase production. Then some joker injects 1g/kg of glucose in to their peritoneal cavity. No one up regulates their glucokinase in 10 minutes, not even Super Rat*. Insulin response is blunted. Hyperglycaemia results.
*Actually Super Rat could do this but she is always busy saving the planet (again) and doesn't have time to help out here.
What would have happened with a few days carb loading in the VLC group before the GTT? Well, we (that "we" includes A&A) know the answer to this from 2006. Did you really think A&A are stupid? How many times do I have to point out that these people are good. Very, very good. They know that to get a "bad" result for VLC you must NOT increase carbs pre glucose load in a GTT.
Does anyone think that neither Axen nor Axen has heard of glucokinase? That would mean they're stupid. They're not, they know that if they allowed 15% carbs for a few days the VLC group would overlay the curve of the 60% carb group. For crying out loud, they published the damned curves themselves!
No. The effect of increased carbs on a VLC is not "unclear" (their word). It adjusts pancreatic insulin secretion to deal with carbs when carbs form a significant part of the diet. That's called physiology!
In summary:
Do A&A have a paradigm to support, a mortgage or two to pay, a living to make, careers to develop?
A few fatties getting injured is of no concern, provided the models can be adjusted to keep the funding coming through.
Will people edging towards type 2 diabetes get injured by a very low carbohydrate diet or will they be injured by A&A's funding success? What if they eat low fat high carbohydrate in the real world? What is hunger?
You decide. Then go eat some fat.
Peter
But not Crisco. Just say no....
Thank you, again, for so adeptly turning over the stones, revealing what is behind the screen, and helping so many of us understand the machinations behind these studies.
ReplyDeleteYour analyses and reports, and your good humor are a happy blessing.
I greatly appreciate your taking the time and making the effort to maintain this blog and give so much of yourself to those of us who could not make heads or tails out of the convoluted reports of these studies.
Hope Super Rat will fly in to show the charlatans what's what. :)
Thank you very much for so adeptly turning over the stones, revealing what is behind the screen, and helping so many of us understand the machinations behind these studies.
ReplyDeleteYour analyses and reports, and your good humor are a happy blessing.
I greatly appreciate your taking the time and making the effort to maintain this blog and give so much of yourself to those of us who could not make heads or tails out of the convoluted reports of these studies.
Hope Super Rat will fly in to show the charlatans what's what. :)
Hi Peter,
ReplyDeleteThis is a very thorough post/analysis.
Since glucokinase "is down regulated in response to carbohydrate restriction," would it make more sense to lower carbs gradually vs cold turkey?
The link to the post with Helen's comment didn't work for me...
Isn't Crisco, canola oil, a polyunsaturated fat?
ReplyDeleteIt would seem then, according to the charts, that a diet high in fats leads to the sugar hanging around the blood longer than a diet high in carbs.
What am I missing?
john, link is fixed, ta.
ReplyDeletenone, the oil was 17% trans fat. It damages your liver which then fails to control systemic hyperglycaemia. The liver should control blood glucose in response to low levels of insulin from the pancreas. Mess with the liver and the pancreas has to work overtime and you end up with systemic hyperinsulinaemia, fat storage and metabolic syndrome. It is essentially hepatic in origin.
Peter
Thank you Peter for setting straight the record on A&A. Really, you should publish your analysis as a comment on their article in the same journal. This way, A&A *might* actually read it, as may some of their colleagues. I'm sure it'll only fall on deaf ears (blind eyes?), but at least it would be in the academisphere instead of just the blogosphere.
ReplyDeleteMaybe the Ancestral Health Society should publish a journal called "Debunk" where all of our bloggy pals can publish their erudite analyses dismantling papers with poorly done designs and inaccurate interpretations...and downright lies.
Aaron, that's an interesting idea. If I wasn't moving house in 3 weeks time I might see if I could get it in to a letter to the editor format. The donkey work's done.... Would need technical refs on glucokinase and carb intake but not too hard...
ReplyDeletePeter
Yes, it's tough to decided which is "better." I made the comment with "stress hormone" levels in mind. If glucokinase is up, and carb consumption is down, are we more "sensitive" to low blood glucose; if glucokinase downregulates along with carb reduction, is there an advantage of preventing high cortisol & adrenalin--either way, it's not that important.
ReplyDeleteOn that subject though, what does long term OD do to fasting adrenaline/epinephrine?
Hi Peter.
ReplyDeleteTalking about diabetes, you might find this video by Dr. Delgado amusing - it shows you how to become diabetic in 6 hours:
http://www.youtube.com/watch?v=_42LfH8veEU
It is the little things about this video that make it so funny; ridiculous, actually. For example, statements to the effect that: "my LDL is so low that it cannot be measured", "the fat in the blood makes it sticky", "I believe my blood glucose will deteriorate throughout the night, and I'll become diabetic".
All of this coming from someone who supposedly is a "doctor".
I wrote a sarcastic post about it, but a few commenters apparently misunderstood my intentions:
http://healthcorrelator.blogspot.com/2010/08/how-to-become-diabetic-in-6-hours.html
Hello, I'm from Brazil.
ReplyDeleteI found your website and wanted to ask, please, for that added the link to my blog for disclosure in order to be partners.
Already added your on my list of partners, ok?
My blog is technology, science and health: http://www.biomedicinaunip.blogspot.com
Thanks!
you will forever be among the top google results for "crisco poisoned"
ReplyDeleteJohn,
ReplyDeleteLong term OD cortisol levels, no catecholamine values:
Cortisol (μg/dL) 10.41 ± (sd)4.74 (median 10.09) Ref range 6.2-19.4
Ned, ah, now there you go! I enjoyed the comments as much as the post and picked up the one from Helen on rats, exercise and glucokinase regulation too. Got a few other refs on that subject too but it's not well written up on Pubmed as yet.
Antispirit, well people do feel pretty rubbish in the first week of Atkins induction and a number of very experienced people, Lutz and Groves come to mind, don't do ketosis as a goal per se. Lutz' approach would never put anyone near ketosis and is a nice level for the long haul in many people....
I went to the paper through a friend being a bit worried by Carb Sane's citation of it. I can see where she (CS) is coming from but once I got in to the full text of the paper it turns out to be supportive of LC eating and suggests that avoiding bolusing yourself with glucose while in near ketosis is a Good Idea. The various adverse adipose tissue distributions and that the rats lose weight better under HC conditions than VLC conditions are things A&A can achieve but I can't fathom (might be to omega 6 content). As I say, A&A are good. The glucose and insulin effects for LC are fine.
But once I got into the history it was all just too funny, or not funny, depending on your point of view. If anyone thinks feeling ravenous on Weight Watchers is fun or healthy...
jon w,
LMAO. Oh, there is one other citation!
Peter
Good analysis. Just one correction: the soleus muscle is not a "typical muscle" in rats since rats are predominantly fast twitch, and soleus is a slow twitch (oxidative) muscle. See also this paper too http://www.ncbi.nlm.nih.gov/pubmed/20086199 which discusses how the soleus in rats preferentially takes up c-18 fatty acids. They picked the soleus because they thought they could get the most damning results that way. I also like this paper discussing the "athlete's paradox" whereby endurance training increase both intramuscular triglycerides and insulin sensitivity. http://ajpendo.physiology.org/cgi/content/full/294/5/E882
ReplyDeleteCynthia
Thanks Cynthia. I have clearly underestimated A&A. I thought they were just very, very good. Not enough "very"s there!
ReplyDeleteI have to say this sort of chicanery actually makes me feel sick on occasions.
What if they hadn't shot themselves in the foot with the 2006 paper? That graph c in 2010 is enough to have anyone reaching for the low fat spread....
Peter
Beautiful post, Peter! I wish I were Super Rat.
ReplyDelete