This paper, which has been sitting on my hard drive for a few years, surfaced on Facebook recently. I gather it has been cited by someone who’s writing requires more ondansetron to read than I currently possess. I’ll just assume it was some sort of “eat LC and the first smidgin of myocardial hypoxia will finish you off” warning, but I’m just guessing and I have every intention of keeping it that way.
The paper itself is very convincing, well written and the protocol extensively justified. The core findings are that a LC diet impairs insulin signalling, depletes myocardial glycogen and results in massive necrosis during reperfusion after a period of myocardial hypoxia. The basic idea is that the lack of glycogen limits substrate for anaerobic glycolysis and failed insulin signalling both impairs glucose delivery from the perfusate and also fails to deliver a number of highly beneficial insulin effects which are independent of GLUT4 translocation.
This is the fate of the LC myocardium. As one of my co workers might say: Dig the hole, choose the coffin.

Obviously, for a LC eater, this is disturbing. The queue for McDougall-ism is over there.
The first thing which I find slightly disturbing is that, in a trial of the Atkins Diet™ (always mention by name), the rats ate more and were significantly heavier than the control rats, within two weeks. I’m not totally certain if I remember correctly, but I thought that the Atkins Diet was used for weight LOSS, not weight gain. Perhaps the authors might have been a little disturbed by this finding too, but apparently it doesn’t need mention. Hmmm.
The Atkins™ like diet is TestDiet 5TSY, no longer manufactured. Table I is abstracted by the authors from the full formula provided by Purina and supplies information on a need-to-know basis.
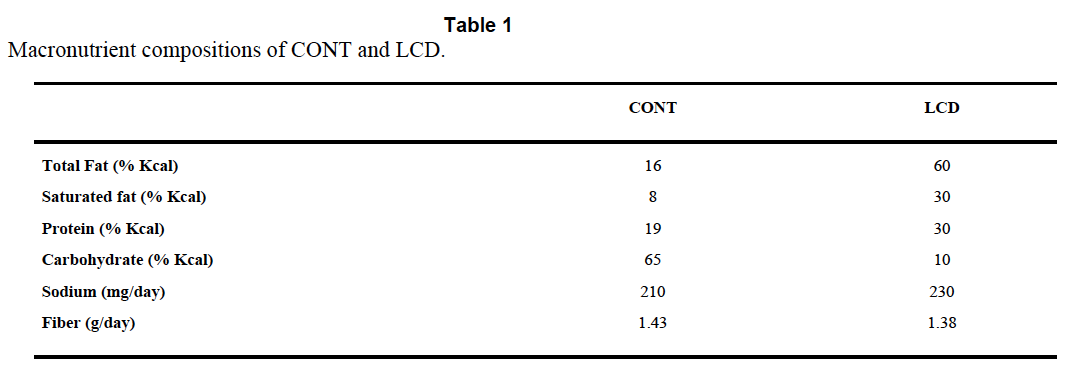
So we know total fat, saturated fat and that “The diets have the same concentrations of essential fatty acids”, i.e. we don’t quite know what the diets were made of. But Purina still will email you a pdf (very promptly) and that gives you this:

There is no mention of Crisco™ by name and no information about the trans fat content, but can you guess how much "Vegetable shortening" is in the control diet? Oh, you guessed!
I know it seems stupid to say this, but if you want to lose weight and/or survive a heart attack, for goodness sake do not choose Crisco or its equivalent as 20% of your calorie intake.
Now, this study does not tell us that a low carbohydrate diet is is good or bad for surviving a heart attack, it's simply not possible to pull that information out due to the lack of control of the variables in the diets. One can only wonder whether the formula of the Atkins Rodent Diet was specifically developed to cause metabolic problems or that somewhere along the line the original Atkins diet suggested a generous consumption of trans fat based vegetable shortening. Maybe I missed this.
I guess you could leave it there and say don't eat vegetable shortening, but there are a whole stack of follow on ideas to this study. There is MASSIVE cardiac necrosis in the LC group of rats. If it is the trans fats, how do they cause this?
One very interesting aspect of the study is the pre-ischaemia depletion of glycogen. These rats are not in ketosis. The doubling of ketone levels from 0.3mmol/l to 0.6mmol/l may well be statistically significant, but is not biologically significant. To go back, yet again, to Veech et al, we need around 5.0mmol/l of mixed ketone bodies to completely replace the insulin signalling system. You can't sidestep insulin resistance with 0.6mmol/l B-OHB. You simply cannot get rats in to a functional level of ketosis with protein at 30% of calories and carbohydrate at 12%. You need carbs near zero and protein limited to < 10% of calories to have rats in nutritional ketosis. Some papers limit protein to < 5% of calories, with minimal carbohydrate.
A period of starvation for rats on the control chow would have tested the hypothesis that it was a lack of glycogen which damaged the myocardium under hypoxia.
My own idea is that the glycogen depletion might be a surrogate for insulin resistance rather than carbohydrate restriction. We have long known that trans fatty acids from partially hydrogenated vegetable oils induce insulin resistance (though not in every study!).
So the next thought is: What sort of insulin resistance?
Are we thinking about an excess of superoxide from complex I, to imitate post prandial hyper caloric insulin resistance? Or are we thinking about the insulin resistance of fasting, when uncoupling results in blunted insulin signalling combined with high oxygen consumption and limited ATP generation?
I like the second idea when applied to this study.
If trans fatty acids, which are structurally similar but not quite identical to saturated fatty acids, allow persistent low level uncoupling outside of the physiological role of the normally structured FFAs it is interesting to speculate that they may continue to allow uncoupling when uncoupling should be utterly and totally banned.
The consequences would be decreased ATP production per unit oxygen consumed. A bit like the findings in Table 3 of this paper. The last column gives you the ATP generated per unit O2 consumed. This would be a disaster under hypoxic conditions. The IF line uses industrial trans fats. The soleus muscle is the mitochondrial dependent one cf the tibialis muscle..
ASIDE: It's worth noting that cytoplasmic ATP is a marked inhibitor of uncoupling but that this is easily overcome by adequate levels of mitochondrial ATP binding within the UCP pore from the end which does not produce a conformational change. Figure 7 gives the details but the main text is really clever stuff (without an agenda, as far as I can see). I'll blog about this paper sometime.

Under this control system the occurrence of falling mitochondrial ATP levels should allow cytoplasmic ATP to immediately shut down the normal uncoupling associated with ketogenic eating and maximise coupled ATP production per unit oxygen when this is needed. The interesting question is whether the uncoupling suspected of transfats persists under low mitochondrial ATP levels. END ASIDE.
You could speculate for hours about what trans fats may or may not do.
This is a very fertile area for idea generation. Ultimately, we don't know what a LC diet based on real Food would do to ischaemic damage in the heart. Maybe it will be as bad as a trans fat based LC (weight gain inducing) diet, maybe less severe.
We are never going to find out what Food does by using "AIN-93G Atkins/Rodent 5TSY" diet based experiments. The rats died in vain, especially as the study buried the possibility of lethal effects from trans fats.
Peter

28 comments:
Peter, even potent Denver-level antiemetics won't protect you from such superficial, mangled scientific interpretation.
Excellent foray into the details, which as we all know, is where the devil lives.
So I guess f*cking with lipid membrane composition ain't good for cellular function, in turn affecting tissue integrity (endothelial vascular tissue here).
I do wonder however if cycling in and out of ketosis has some inherent metabolic "switching cost". Of course, we are clearly adapted to do so, but that doesn't guarantee 'costless' transitions above & beyond a certain number/threshold. [This does not worry me, but it may tell us something more about the advantages or drawbacks of of dietary ketosis]
Two thoughts:
1. It would seem relevant to consider the impact of the diets on the rate of ischaemic hypoxia as well. Even if the LC diet fairs worse when hypoxic (which I could buy), if it reduces the incidence of hypoxic conditions as well, the net benefit would still be there. Also, I was under the impression that complete glycogen depletion when low carb was unusual.
2. Re: trans fats. I seem to recall that trans-fats (specifically elaidic acid) cannot be completely beta-oxidized because of the location of their trans-bond, and results in a build up of intermediaries during beta-oxidation and ultimately cell death. Whereas other trans-fats (vaccenic and cla) have the trans bond in a position where it can be completely oxidized, and don't have the negative effects.
@IcedCoffee - Regarding your elaidic acid comment, it would also increase CETP activity which would decrease HDL, thus possibly limiting HDL repair mechanisms. Which under hypoxic conditions would be even worse.
Hi !
what do you think about all the GIK litterature ? bullshit ?
Peter, another thing you might want to add to the article is that they also used lard and I highly doubt they rendered their own. In which case it's almost universally hydrogenated, thus adding even more trans-fats. So even the ~20% of calories you state from 'Vegetable Shortening' understates the amount of trans-fat in the mouse chow.
http://soursaltybittersweet.com/sites/soursaltybittersweet.com/files/ThingsThatMightKillYouVolume1Transfats_23E1/lard.jpg
Peter, what are your thoughts on berberine:
For example I know that you are a fan of physiological insulin resistance, and this substance is claimed to improve insulin sensitivity from receptor cells. Would taking berberine make one 'too insulin sensitive' ? Or is it a case where it is beneficial ?
Thanks. :)
Zorica, I was also interested in Berberine for the same reason but Jenny from Blood Sugar 101 is scathing of it and believes it may be harmful. A commenter also provides links to studies relating to DNA damage but I would certainly be interested in Peter's view...http://www.fda.gov/aboutfda/centersoffices/oc/officeofscientificandmedicalprograms/nctr/whatwedo/nctrpublications/ucm363503.htm
1. Berberine, are potent inducers of DNA damage
2. Berberine-treated cells, DNA damage was shown to be directly associated with the inhibitory effect of topoisomerase II (an essential enzyme for DNA replication) and a key element for cell division and gene duplication fidelity.
Theoretically, this means any proliferating or newly dividing cells could subject to the cell division damaging inhibited by Berberine. Targeted delivery system for this compound may be preferred not to elucidate the long term damages of gene duplication.
@LomaxZ,
but if fats are fully hydrogenated, not partially hydrogenated (trans-fats), would it be accurate to say than that a complete hydrogenation is the synonym of a saturation?
Hi nfkb0,
I've been interested in GIK for years, mostly as it might make the management of DKA significantly easier. Practically I never deal with ischaemic heart disease so it has no appeal there. It's use is very much based around Ling's structured water ideas which I feel are correct but very difficult to integrate with the more superficial level of physiology which my brain is locked in to.
The people who use it are working at my type of superficial level too, cells need ATP, drive glucose in with insulin and try not to kill your patient with hypokalaemia. The studies seem to show that it works well if you are a believer and that it is very easy to arrange a non-believer study design to have it fail. So the benefits are probably not huge.
I would guess it might well be helpful in a transfat based experiment (i.e. much of the world, especially the USA) where the loss of downstream insulin effects on the ETC are lost through failure of insulin to act appropriately...
ZomaxZ, wow, USA food!
Zorica and Jasmin, that would need a ton of reading. Metformin is lethal in overdose or if you use more potent analogues. The lifespan enhancing effect of metformin can be equally well generated with rotenone, yet high dose rotenone is the standard method for generating a Parkinsons-like model for drug testing. Where does berberine fit in to this spectrum? Ask me when 100,000 people have taken it for 30 years at some standardised dosage protocol. Any drug with major metabolic effects will have major toxicity when you get it wrong. My garden is full of foxgloves but the few patients I ever digitalise get very, very controlled dose rates with routine blood digoxin measurements during stabilisation. Not that I can remember the last time I digitalised a patient!
Galina, if only what they say was done is what was actually done……..
Peter
Caffeine is pretty good for breaking DNA, but coffee prevents liver cancer. Berberine naturally occurs in a few herbs; it is related to opiate precursors that occur in many more, none of these are highly toxic, many are useful. But if you use a berberine supplement the dose is higher than a human used historically, and the effect is not being modified by other components of the herb. (similar to digitalis; toxicity when using the herbal extract was supposedly easier to identify and avoid than when using digoxin).
I suggest olive leaf extract as a more food-like substitute for berberine if the goal is lowering GNG.
@Galina - It's not totally true to say that hydrogenation is a synonym of saturation; however, if you fully hydrogenate, then it is true. I'm not aware of any commercially available lard that is fully hydrogenated, but if it were it would end up with little to no trans-fat and a lot of stearic acid since lard contains a lot of oleic acid.
Thank you, LomaxZ, for ansvering my question.
I got curious about the change started to notice in stores on labels of re-formulated products which previously contained trans-fats, like peanut butter, but nowadays the list of ingredients often contains hydrogenated or even fully hydrogenated vegetable oils. Armour lard in my local groceries store contains Lard and Hydrogenated lard. I don't buy that staff anyway.
Berberine mimics the effects on the SNS of cold thermogenesis. It is the same of how niacin mimics a ketogenic diet by its effects on NAD+
HI Peter, thank you for you answer.
Actually i'm not a super strong believer of the GIK cocktail to improve cardiac ischemia. The Immediate trial is the latest stuff and its primary endpoint is negative.
But as an anesthesiologist in human medicine, i often face myocardium ischemia and after a surgery i'm more prone to give gik than a super-dangerous cocktail of antiplatelets agents and anticoagulants that cardiologists (and big pharma) love.
I would also say that GIK costs nothing, what about the new *grel stuff and the even newer antiinflammatory *mab stuff which are in the pipeline...
I also think that the K in GIK is very important, i give some hints about K in this french post : http://www.nfkb0.com/2014/06/09/mon-ami-le-potassium/ (hope web translators help)
Finally i love your blog, i've discovered it a few weeks ago and i try to understand it patiently :) I'm not turning into a LCHF eater because i'm a slim but big breadholic french ;) However i love your explanations and i'm reading more and more basic physiology (and Lane books) to understand your blog and i like it :)
PS i'm Rémi F on FB.
PPS when will you open a twitter account ? Twitter is a super tool
Peter said "Ask me when 100,000 people have taken it for 30 years at some standardised dosage protocol."
This is wisdom. Exactly why I don't take anything but metformin and low carb for my Type 2 diabetes. Tweak one metabolic process with a drug (and yes, refined berberine is a drug) and where does it end? I don't want to be the test case. Fools rush in where angels fear to tread.
Regarding GIK for CVD, PAD, or CVA: I sent Peter Sinclair's 2013 paper on pseudo-hypoxia a few blogs back. It perfectly describes what Ling said about GIK long ago. Quick summary for those interested:The Sinclair paper linked here before shows that mitochondrial dysfunction is cause by a metabolic shift due to altered epigenetic redox changes in cell water or plasma. This results Warburg-type metabolism under pseudo-hypoxic states in cell water. This is where protons are more plentiful than electrons from ETC. Peter has beautifully laid this out here over 30 blogs. Warburg metabolism are fully reversible with the supplementation of NAD+ precursors (niacin) or a DHA laden ketogenic diet and metformin. Ketosis also happens to replenish NAD+ for the nucleus! Ketosis is protective because it allows passage of electrons and protons from fats (FFA) to make some ATP and salvage the mitochondria damaged by the metabolic redox shift these cells or tissues possess to keep them from oncogenesis. It promotes senescence instead. If the mitochondria is not trashed it can recycle itself using autophagy. Ketogenic diets have also been shown to aid deep sea divers and special force soldiers overcome situation where they face chronic hypoxia. Ketogenic diets help prevent brain cancer and improve cardiac function in heart disease because it improves NAD+ ratio's fast at cytochrome one. (http://www.nature.com/nature/journal/v487/n7408/full/487435a.html) There are many reports that a sick brain does not really use glucose (you'd never know that reading the blogosphere Guyenet, Kresser or Jaminet) but changes it to lactate which neurons love to use as a fuel with fats. Here is where saturated fats have a protective role. The humans brain loves fats and lactate fuels together. The heart also loves this combo because both tissues are loaded with mitochondria that have been shifted. Moreover, but guess what also likes this combo of lactate and fats? All other tissues in your body do. So when you eat fat you will not get CVD, cancer, or get fat. Peter knows the data on lactate because he has blogged on it. Lactate usage by the brain and heart appears to be the best way of postponing apoptosis (cell suicide), short of abandoning your brain/heart mitochondria altogether. This is why CVD walks hand and hand with neurodegenerative disorders because both tissues have high mitochondrial dependency. Glucose use comes in as a second choice in the heart and brain when they have redox issues. GIK is hogwash for CVD, PAD and CVA because of the "GI portions" of this equation. Ling showed K+ was the key to water structure inside a cell. Gerald Pollack extended Ling's work, by showing in hydrophilic nafion tubes naturally create adiabatic protons flows by charge separting water.
He extended Ling's work. But the K+ is the key for the heart. K+ links water molecules to ATP molecules stochastically. This is what Gilbert Ling proved 60 years ago and no one seems to know about it. Potassium levels tell you about the relationships to ATP. For every 0.3 mEq below 3.8 mEq that potassium is on a standard blood lab draw, means there is 100 mEq deficit inside a cell. The atomic size and its redox potential is huge for potassium “gluing of water” for it to function as the optimal electrical adapter to transfer energy throughout the cell coherently. ATP is designed to unfold proteins fully to open their carbonyl and imino side chain groups on all amino acids to intracellular water. This action allows binding and polarization to separate water into subatomic particles that are positively and negatively charged. This action is called building or expanding the exclusion zone (EZ) of water. Pollack's experiments showed these effects. Ling proved by experiment that each molecule of ATP in a cell controls 8,800 water molecule binding sites and 20 potassium ions to allow water to become structured inside every cell of your body. The first step in photosynthesis and ox/phos is the charge separation of water. Ling was the first to realize K+ linked water to the ATPase. So when you have altered poor K+ your dehydrated and the interior or your cell is pseudo-hypoxic and this causes the redox shift of the mitochondria.
I went into the detail of how Ling dovetails with Sinclair and Pollack here @ Bill's blog: http://caloriesproper.com/?p=4903#disqus_thread
Ilaine, I have seen too many drugs come and go over the last 30 years to get too excited about anything new. The latest NSAID has me rushing to observe the effects on my co-worker’s patients before I prescribe. About a year for most drugs, five years for an NSAID!
Jack, we both realise that lactate is the preferred fuel for neurons. I have a set of links from Edward and an email query to tie together on this.
And to Jack and Rémi,
I came up through the 1980s without in-house K+ measurements, in a small rural practice. I can remember poring over the ECG of critically ill patients looking for spiked T waves and flat P waves. The Vetlyte 8008 in-house analyser was a godsend. I also remember a sepsis patient (post pyometra resection) which went from ambulant through hind limb ataxia to quadriparesis in just over an hour. Some KCl fixed it equally rapidly. The potassium analyser paid for itself that day.
It’s only as I came to metabolism, insulin and Ling that I started to ask deeper questions. The structured nature of water in modern cells is a given. I have a paper suggesting ATP is moved through structured water using chains of adenylate kinase and an ATP/AMP:2ADP shuttle system. Diffusion does not seem to be where it’s at.
But, at the most basic level, I cannot see ATP as primal. Jack, I know you see Ling and Lane/Martin’s ideas as incompatible. I cannot see anything other than they must be reconciled as two views of the same system. If, as I do currently, you go with Lane/Martin, you are looking at the core starting points to metabolism as being reduced ferredoxin based. Probably as FeS, obviously without the protein carrier structure (http://www.nick-lane.net/Lane-Martin%20Cell%20origin%20membrane%20bioenergetics.pdf). The use of reduced ferredoxin is still core to the most evolved organisms on earth, the methanogens and acetogens. While they have clearly accepted ATP, they still have reduced ferredoxin at the core of their energy metabolism. While they are highly sophisticated, extremely “evolved” organisms, they still give us the best insights as to where metabolism probably started. I would agree ATP is a very early development (the ATP synthase complex clearly predates the differentiation of methanogens and acetogens from each other. ATP synthase developed before the formation of lipid membranes). So, to me, metabolism and synthesis had to be on-going well before ATP evolved. Some other molecule would need to be put forward as the as the structuring agent to cell water before the highly developed molecule of ATP came along. Lane/Martin’s ideas put in place a limited metabolism within a physically limited structure, with continuous energy throughput.
While a great deal has changed since the origin of life I see the complex protein/water/potassium/ATP interaction as being subsequent to its development. For Ling to be primal I would want an explanation of how structured water gives us proto-methanogens to become eukaryotes with proto-acetogens to become the mitochondria. These ideas seem to drop easily out of Lane/Martin but I struggle to see how Ling’s ideas would explain them, not that Ling’s ideas do not have explanatory power in their own right.
As I say, I feel they are views of the same phenomenon…
Peter
Peter I agree........your missing piece is Gerald Pollack. Read his book the fourth phase of water and you will see how his experiments built upon Ling's ideas and extended them and totally explains why Mitchell's ideas are wrong. Ling gave us the thermodynamic reason Mitchell was wrong but Ling could not explain precisely the mechanism of how water structures. Pollack does. IT solves Lane's problems at the smokers in the ocean too. Infrared radiation requires no sunlight for charge separation in water.
I've watched Pollack's lectures, I still don't know how to go about racking up a better exclusion zone and cranking up my negative charges.
Dunno, maybe just vigorously stir my water and leave it in the sun for a while, maybe it'll spontaneously develop higher ratios of H3O2.
Jack, Lane/Martin look at acetogens and methanogens, nowadays using reduced ferredoxin to reduce CO2. This reduced ferredoxin is hard to come by and today the trick is turned by using electron bifurcation, i.e. BOTH electrons from H2 are used, at the same time, to generate the necessary reduced ferrodoxin. Without reduced ferredoxin CO2 is not going to be reduced to CO as the needed redox potential is -520mV.
I don’t see how you can have this happening pre-genes and pre-proteins, using an IR induced aqueous exclusion zone potential of -200mV.
Lane/Martin posit disordered mackinawite with a Eh of ~300mV at pH 7.5, becoming more negative by with rising pH, i.e. under alkaline vent conditions it may well be able to supply a redox potential of nearly -600mV needed to reduce CO2 to CO. This is at an iron/sulphur boundary between acidic CO2 rich ocean and an alkaline H2 rich serpentinisation effluent.
I struggle to get these sorts of processes from some infra red photons acting on water to expand/contract a structured water exclusion zone. If infra red could allow hydrogen to reduce CO2 under biological conditions the world would be teeming with IR photosynthetic organisms, which it’s not… I may have missed some of Pollacks better points as I’m working from his 2009 paper http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680624/
I have no problem with structured water on FeS surfaces, I have no doubt it is of consequence, but I still don’t see how it might replace Lane/Martins arithmetic.
Peter
I think when you read all of his ideas and see all the experiments he has done in one place you will get it. The high pH and large exclusion zone are congruent.......the high the pH the lower the proton amounts. The more electrons present the more negative the charge and the more dense water is around those smokers to provide the energy to drive a zero entropy self assembly. The earliest pathways.....like the reducing pathways could all be run adiabatically when you consider the massive charges in water that is constantly restored. It can be done by the sun or by IR heat.
Phillpa Wiggins work on water density and action takes Pollack's ideas even further.......
Peter, when someone has a higher fasting glucose on LC or keto, is that higher sugar from GNG? I know there's beneficial physiological insulin resistance, so if it is GNG, then that is a good thing?
I'm interested to know, and would like to know if it's another mechanism (ketone bodies interacting here?)
Thanks.
Zorica, I've not really given that a huge amount of thought. Resisting insulin in the periphery and in the liver might both be a normal aspect of ketogenic diets. Even the brain might be involved in fine tuning blood glucose, as it undoubtedly always is...
Peter
This just figures though, the diet scene tells us to avoid carbs completely but that's not true, we need them just as much as we need certain fats and oils, it's just like anything else, too much of a good thing is bad. The science is helpful to see what's behind the reasoning but it just seems like common sense should prevail.
Post a Comment