Many observational studies associate prostate cancer with markers of metabolic syndrome. Which gives us the omega3/trans fat paradox, well discussed in several places around the net.
Here's a similar prostate paradox.
How come these two exceptions buck the trend? Here's a random thought:
Let's assume prostate cancer is related to chronic hyperinsulinaemia, a reasonable idea, ie it is "metabolic syndrome of the prostate".
Conversely, castration is a component of conventional prostate cancer treatment.
Getting to the chemical-castration stage of metabolic syndrome might well be prostate cancer protective.
Omega 3 fats probably slow progression of metabolic syndrome, trans fats probably accelerate it.
If you want to get to the castration level of metabolic syndrome as fast as possible, to maximise this prostate benefit, never forget to ask for your favourite lipotoxin by name.
For metabolic castration you should always ask for Crisco.
Peter
Alternatively I have a couple of bricks available. It's an old anaesthetist's joke:
Surgeon: "I don't need to use anaesthesia for castration."
Anaesthetist: "Really, what's your technique?"
Surgeon: "I have these two bricks and I smash them together on the testicles."
Anaesthetist (aghast): "Doesn't that hurt?"
Surgeon: "Only if you get your thumbs in the way."
Saturday, April 30, 2011
Monday, April 25, 2011
Diabetic nephropathy and the lost Swede
Chris over at Conditioning Research forwarded me the link to the PLoS paper demonstrating partial reversal of diabetic nephropathy in a couple of mouse models. This isn't exactly a world shattering finding as anyone with diabetes who is not eating a mildly ketogenic diet probably has shares in dialysis machines or is being grossly mismanaged.
Anyway, the first thing to do with a paper like this is to check whether the authors cited Nielsen's 2006 case report of a human being having their diabetic renal failure halted and partially reversed. I mean, this might be relevant...
They didn't.
The Swedish group simply fixed a patient without a mouse model in sight. They got ignored for their temerity. Shocking to fix a human without the death of a single leptin deficient mouse, but there you go. And it's not so hard to do either............
As a complete aside:
It turned out to be interesting to go back and see where the mouse folks were coming from. They cited this paper.
Here is part of figure 6, the line to follow is the open triangles.

Up to day 84 a high fat diet was fed. As happens so often, the high fat diet is 31.7% sucrose/maltodextrin by weight and (gasp) 20.7% lard.
From day 84 onwards these lazy, greedy porkers of mice were switched to a diet which was 47.5% lard and, utter horror, 19.95% butter. Of course this is not really a high fat diet as it has no sucrose or maltodextrin...
Look at the weight drop to below (ns) that of the mice fed crapinabag throughout........
Obviously this must be the satiating effect of protein, so often cited by idiots as the reason for weight loss of LC diets. Except it's not, the ketogenic mice had the lowest protein intake, 9.5% by weight cf 24% in the crapinabag and HF diets. That is very low in protein.
Here are the actual diets in Table 1:

A far more plausible explanation is that ketosis induces dissatisfaction in these mice concerning their body image due to their obese state so they then started to cut calories and go to the gym every night. Duh.
Now please don't make me put up the fasting insulin levels. Aw, okay, you twisted my arm.
Edit: I noticed that these are the FED insulin levels, we don't get fasting levels in the paper...

No comment.
Peter
Anyway, the first thing to do with a paper like this is to check whether the authors cited Nielsen's 2006 case report of a human being having their diabetic renal failure halted and partially reversed. I mean, this might be relevant...
They didn't.
The Swedish group simply fixed a patient without a mouse model in sight. They got ignored for their temerity. Shocking to fix a human without the death of a single leptin deficient mouse, but there you go. And it's not so hard to do either............
As a complete aside:
It turned out to be interesting to go back and see where the mouse folks were coming from. They cited this paper.
Here is part of figure 6, the line to follow is the open triangles.

Up to day 84 a high fat diet was fed. As happens so often, the high fat diet is 31.7% sucrose/maltodextrin by weight and (gasp) 20.7% lard.
From day 84 onwards these lazy, greedy porkers of mice were switched to a diet which was 47.5% lard and, utter horror, 19.95% butter. Of course this is not really a high fat diet as it has no sucrose or maltodextrin...
Look at the weight drop to below (ns) that of the mice fed crapinabag throughout........
Obviously this must be the satiating effect of protein, so often cited by idiots as the reason for weight loss of LC diets. Except it's not, the ketogenic mice had the lowest protein intake, 9.5% by weight cf 24% in the crapinabag and HF diets. That is very low in protein.
Here are the actual diets in Table 1:

A far more plausible explanation is that ketosis induces dissatisfaction in these mice concerning their body image due to their obese state so they then started to cut calories and go to the gym every night. Duh.
Now please don't make me put up the fasting insulin levels. Aw, okay, you twisted my arm.
Edit: I noticed that these are the FED insulin levels, we don't get fasting levels in the paper...

No comment.
Peter
Yesterdayday was first meat day
Edit: Today was fillet steak, OK so long as the piece is big enough to be sucked on without getting it all in her mouth at once...

Apparently babies are revolted by meat, just ask any vegan idiot



Peter

Apparently babies are revolted by meat, just ask any vegan idiot



Peter
Sunday, April 17, 2011
Palmitic acid: the horror never ends speculation
Back in her PhD days my wife attended a seminar presented by a visiting researcher on some aspect of the inflammatory cascade. It was very technical and focused around the interaction of a certain ligand with its receptor at some critical juncture in whatever process they had devoted the last n years of their life to studying.
The ligand was all-cis-docosa-4,7,10,13,16,19-hexa-enoic acid. No one in the room had any idea what this stuff was, certainly not the extremely intelligent presenter, other than as a molecular key to a molecular lock. It's a stock lab reagent purchased in research grade purity from any one of a number of suppliers. You could equally order cervonic acid.
At the level of reductionism these people can work at there is no need to be aware that all-cis-docosa-4,7,10,13,16,19-hexa-enoic acid is available in gel caps from Holland and Barrett or is present in the nearest can of sardines as the more familiar DHA.
So imagine you are some newbie PhD student. You walk in to the lab and are handed a reading list a mile long. The lab has certain research lines you are going to slot in to, particularly focused around inflammasome activation by fatty acids. You got the post because you had picked up extensive experience with cell culture and inflammation research based around both endotoxin and asbestos, plus a track record of multiple Nature publications from your undergraduate work.
The lab you walk in to has cells in culture which go ballistic on exposure to utterly physiological concentrations of palmitic acid. At least six widely differing cell types behave in exactly the same way. This looks like a generic effect and puts palmitic acid up there with asbestos as a proinflammatory agent. You switch to Flora that very lunch time, and spread it thinly too.
The lab also has an animal house in the basement. The rats are either fed a standard lab chow or a red coloured greasy type of pellet oozing fat. The lab techs feed and water the ratties. Your job is to compare molecular aspects of white blood cell inflammasome activation as the high fat rats get fatter over the weeks. Once a fortnight someone brings you a blood sample to work with but, apart from that, you will never see the rats again...
What do you question? EVERYONE knows that eating fat makes you fat. Fat is fat. Do you give a monkey's about EXACTLY what is in the pellets which stain the tech's hands red when they do the feeding? It's a standard obesogenic high fat diet from www.testdiets.com. All obesity research uses it or something similar...
Would you sit down and work out whether the hydrogen atoms on either side of the central double bond of one type of fatty acid in one constituent of the 5TJN are aligned on the same side or on opposite sides of the bond? You know, cis vs trans configuration...
It's sloppy. It's possible. People will really be able stand up and say, as Ting does:
"The simple message is to avoid fatty foods as much as possible."
They probably have no doubts. They believe. It's complete bollocks of course. But I have this concept of how things work...
Peter
The ligand was all-cis-docosa-4,7,10,13,16,19-hexa-enoic acid. No one in the room had any idea what this stuff was, certainly not the extremely intelligent presenter, other than as a molecular key to a molecular lock. It's a stock lab reagent purchased in research grade purity from any one of a number of suppliers. You could equally order cervonic acid.
At the level of reductionism these people can work at there is no need to be aware that all-cis-docosa-4,7,10,13,16,19-hexa-enoic acid is available in gel caps from Holland and Barrett or is present in the nearest can of sardines as the more familiar DHA.
So imagine you are some newbie PhD student. You walk in to the lab and are handed a reading list a mile long. The lab has certain research lines you are going to slot in to, particularly focused around inflammasome activation by fatty acids. You got the post because you had picked up extensive experience with cell culture and inflammation research based around both endotoxin and asbestos, plus a track record of multiple Nature publications from your undergraduate work.
The lab you walk in to has cells in culture which go ballistic on exposure to utterly physiological concentrations of palmitic acid. At least six widely differing cell types behave in exactly the same way. This looks like a generic effect and puts palmitic acid up there with asbestos as a proinflammatory agent. You switch to Flora that very lunch time, and spread it thinly too.
The lab also has an animal house in the basement. The rats are either fed a standard lab chow or a red coloured greasy type of pellet oozing fat. The lab techs feed and water the ratties. Your job is to compare molecular aspects of white blood cell inflammasome activation as the high fat rats get fatter over the weeks. Once a fortnight someone brings you a blood sample to work with but, apart from that, you will never see the rats again...
What do you question? EVERYONE knows that eating fat makes you fat. Fat is fat. Do you give a monkey's about EXACTLY what is in the pellets which stain the tech's hands red when they do the feeding? It's a standard obesogenic high fat diet from www.testdiets.com. All obesity research uses it or something similar...
Would you sit down and work out whether the hydrogen atoms on either side of the central double bond of one type of fatty acid in one constituent of the 5TJN are aligned on the same side or on opposite sides of the bond? You know, cis vs trans configuration...
It's sloppy. It's possible. People will really be able stand up and say, as Ting does:
"The simple message is to avoid fatty foods as much as possible."
They probably have no doubts. They believe. It's complete bollocks of course. But I have this concept of how things work...
Peter
Thursday, April 14, 2011
Palmitic acid: the horror never ends addendum
Okay, Victoria sent me the full pdf.
This group used 0.2mmol/l or 0.5mmol/l palmitate conjugated to bovine serum albumin. All other fatty acids were completely excluded. No semblance of physiological mixtures were involved.
But guess what, they had a living mouse model too!
Now you have to be wondering exactly how they managed to get a mouse to have 0.5mmol/l of palmitate in its bloodstream, to the exclusion of all other fatty acids, during a glucose tolerance test. After all, their test tube model used pure palmitate, surely they used the same conditions in their mice? This is a Nature paper after all.
How did they perform this near miracle? Well the methods section (when you finally find it tacked on to the end of the paper, an afterthought down beyond the references) doesn't mention any attempt to measure live mouse fatty acids at all. They didn't. WTF, this got published in Nature!
The diet used was good old commercial 5TJN. When I downloaded the composition pdf from the Test Diet website to my laptop it said I'd already downloaded it some time before..... It's popular!
Here's the link, it won't embed:
www.testdiet.com/PDF/5TJN.pdf
How much sugar would you like with your Crisco? Remember, always ask for your favourite lipotoxin by name...
NO NO NO.
JUST SAY NO.
Say no to Crisco.
As so often happens, this paper details feats of molecular and cellular manipulation of breathtaking complexity. How can anyone be capable of doing this and yet be so stupid? Awesome!
Peter
And it gets worse. The stats were done on "Prism 5.0 for Macintosh". OMG they're Mac users. It shouldn't be allowed. Their laptops should be confiscated forthwith. Now. I'll have them please.
This group used 0.2mmol/l or 0.5mmol/l palmitate conjugated to bovine serum albumin. All other fatty acids were completely excluded. No semblance of physiological mixtures were involved.
But guess what, they had a living mouse model too!
Now you have to be wondering exactly how they managed to get a mouse to have 0.5mmol/l of palmitate in its bloodstream, to the exclusion of all other fatty acids, during a glucose tolerance test. After all, their test tube model used pure palmitate, surely they used the same conditions in their mice? This is a Nature paper after all.
How did they perform this near miracle? Well the methods section (when you finally find it tacked on to the end of the paper, an afterthought down beyond the references) doesn't mention any attempt to measure live mouse fatty acids at all. They didn't. WTF, this got published in Nature!
The diet used was good old commercial 5TJN. When I downloaded the composition pdf from the Test Diet website to my laptop it said I'd already downloaded it some time before..... It's popular!
Here's the link, it won't embed:
www.testdiet.com/PDF/5TJN.pdf
How much sugar would you like with your Crisco? Remember, always ask for your favourite lipotoxin by name...
NO NO NO.
JUST SAY NO.
Say no to Crisco.
As so often happens, this paper details feats of molecular and cellular manipulation of breathtaking complexity. How can anyone be capable of doing this and yet be so stupid? Awesome!
Peter
And it gets worse. The stats were done on "Prism 5.0 for Macintosh". OMG they're Mac users. It shouldn't be allowed. Their laptops should be confiscated forthwith. Now. I'll have them please.
Wednesday, April 13, 2011
Palmitic acid: the horror never ends
Chris forwarded me a link to this study. Read about inflammasones in tissue culture and quake. Here is the relevant line:
"These findings provide insights into the association of inflammation, diet and T2D."
It gets even better. Here is the best line from the press release:
"These results support the idea that inflammation plays a role in chronic disease," says Ting. "The simple message is to avoid fatty foods as much as possible."
OK, you take isolated cells, bathe them in 2mmol palmitic acid and they become unhappy. This is supposed to have something to do with eating a high fat diet?????
Just for fun I'm going, in my head, to eat some (gasp, horror) palmitic acid. Please don't do this at home, you probably don't want to inflame your inflammasomes.
I'm looking through my refrigerator for some palmitic acid but I notice that all there is in my fridge is Food. Bugger. What comes closest? Maybe butter??? Butter is undoubtedly Food, but it does have rather a lot of palmitic acid. Let's give it a try.
Half a pound of butter, here I come. Mmmmmmm. Nice. Yummie.
Now let's measure my blood palmitic acid levels . OOOOOh, post prandial triglycerides are up! Right on, I'm gonna die, some time soon. But what about the acid, the pamitic acid?
Ah, FFAs are also up up up. Success! 500, 600, 700, yes, 800micromol/l. If I really am in luck I might make that 2000micomol/l hit and drop right in to the inflammasome mediated diabetes zone. You know, that palmitic acid trip to nowhere.
Oh, but except for feeling a bit nauseous from all that butter in one go, I feel fine. Perhaps because I don't really have 2mmol/l palmitate in my blood stream after all. Double bugger. It seems like there is major, like MAJOR, contamination of my blood palmitate with oleate. Some is from the butter, some is from my own bloody liver cocking up the experiment. Using delta 9 desaturase to drop the occasional double bond in to long chain saturated fats ensures normal physiology.
Now, if I wasn't such a cheapskate I'd shell out the ackers to see if Ting et al used mixes of palmitate and oleate as well as either fatty acid in isolation. We know from the abstract that oleate does not inflame your inflammasomes... But I am a cheapskate, so I won't. Instead I'll go to this study:
"Low concentrations of oleate (0.1mM) completely inhibited palmitate-induced oxidative stress, SAPK activation, and apoptosis."
That's it, one tenth of one millimole of oleate completely negates the adverse effects of isolated palmitate.
Maybe check this one:
"Oleate alone did not cause mtROS generation and mtDNA damage, and its addition to palmitate prevented palmitate-induced mtDNA damage, increased total ATP levels and cell viability, and prevented palmitate-induced apoptosis and inhibition of insulin-stimulated Akt (Ser(473)) phosphorylation."
I could go on. No one, ever, at any time, has 2mmol/l of isolated palmitate in their bloodstream. A whiff of oleate is completely protective against the evil intentions of a researcher with a block of palmitate when viewed from the bottom of a test tube. It's called physiology. We are evolved to work this way. Knock out delta 9 desaturase and things become quite fun, but that's another story!
Citing the existing literature doesn't get you a Nature publication. Nor does it allow you to write press releases of utter stupidity to support low fat eating while simultaneously keeping yourself off the dole.
Peter
"These findings provide insights into the association of inflammation, diet and T2D."
It gets even better. Here is the best line from the press release:
"These results support the idea that inflammation plays a role in chronic disease," says Ting. "The simple message is to avoid fatty foods as much as possible."
OK, you take isolated cells, bathe them in 2mmol palmitic acid and they become unhappy. This is supposed to have something to do with eating a high fat diet?????
Just for fun I'm going, in my head, to eat some (gasp, horror) palmitic acid. Please don't do this at home, you probably don't want to inflame your inflammasomes.
I'm looking through my refrigerator for some palmitic acid but I notice that all there is in my fridge is Food. Bugger. What comes closest? Maybe butter??? Butter is undoubtedly Food, but it does have rather a lot of palmitic acid. Let's give it a try.
Half a pound of butter, here I come. Mmmmmmm. Nice. Yummie.
Now let's measure my blood palmitic acid levels . OOOOOh, post prandial triglycerides are up! Right on, I'm gonna die, some time soon. But what about the acid, the pamitic acid?
Ah, FFAs are also up up up. Success! 500, 600, 700, yes, 800micromol/l. If I really am in luck I might make that 2000micomol/l hit and drop right in to the inflammasome mediated diabetes zone. You know, that palmitic acid trip to nowhere.
Oh, but except for feeling a bit nauseous from all that butter in one go, I feel fine. Perhaps because I don't really have 2mmol/l palmitate in my blood stream after all. Double bugger. It seems like there is major, like MAJOR, contamination of my blood palmitate with oleate. Some is from the butter, some is from my own bloody liver cocking up the experiment. Using delta 9 desaturase to drop the occasional double bond in to long chain saturated fats ensures normal physiology.
Now, if I wasn't such a cheapskate I'd shell out the ackers to see if Ting et al used mixes of palmitate and oleate as well as either fatty acid in isolation. We know from the abstract that oleate does not inflame your inflammasomes... But I am a cheapskate, so I won't. Instead I'll go to this study:
"Low concentrations of oleate (0.1mM) completely inhibited palmitate-induced oxidative stress, SAPK activation, and apoptosis."
That's it, one tenth of one millimole of oleate completely negates the adverse effects of isolated palmitate.
Maybe check this one:
"Oleate alone did not cause mtROS generation and mtDNA damage, and its addition to palmitate prevented palmitate-induced mtDNA damage, increased total ATP levels and cell viability, and prevented palmitate-induced apoptosis and inhibition of insulin-stimulated Akt (Ser(473)) phosphorylation."
I could go on. No one, ever, at any time, has 2mmol/l of isolated palmitate in their bloodstream. A whiff of oleate is completely protective against the evil intentions of a researcher with a block of palmitate when viewed from the bottom of a test tube. It's called physiology. We are evolved to work this way. Knock out delta 9 desaturase and things become quite fun, but that's another story!
Citing the existing literature doesn't get you a Nature publication. Nor does it allow you to write press releases of utter stupidity to support low fat eating while simultaneously keeping yourself off the dole.
Peter
Saturday, April 02, 2011
Fasting insulin and weight loss and calories-in vs calories-out
I had this exchange in the comments on a previous post:
Frank said...
Hi Peter. I'd say that I pretty much agree with your post. Insulin and caloric deficit are not mutually exclusive, ie, low-insulin could enhance fat loss on a caloric deficit or, looked from another perspective, a caloric deficit could enhance fat loss if someone has low insulin level. I have only one question for you. For the sake of it lets make thing black and white. What do you believe is the most important thing to do, in order to achieve weight/fat loss a) be in a caloric deficit (your insulin level does not matter much) b) having a low-insulin level (it does not matter much if you're in a caloric deficit or not). Again, in real life, I don't believe they exclude each other, but if you could fix only one to have a weight loss, which one would you fix? Calories or insulin? The way I see it is that, as you stated, insulin inhibits lipolysis, but more lipolysis does not equal more oxidation. It still has to be matched to energy expenditure. In that case, calories would be the most important factor. That's my point of view and it could be wrong. I'm just wondering if you agree to some degree with it, because reading your post, I get the idea that you do. Thanks for your time.
Peter said...
Ah Frank, now there is a question. Without caloric deficit (and I want uncoupling proteins, sleeping metabolic rate, spontaneous movements, etc, etc, etc, everything, accounted for) there will be no weight loss. But, in real life, if I could only alter just one, it would be insulin. I would expect no weight loss but I would expect improved health. What else matters?
There is a flaw in the answer I gave to this question. It's working at the Noddy level of calories-in vs calories-out.
The Noddy approach is perfectly adequate to explain the findings of GnK's paper (PR's weight loss excepted, if she genuinely ate all she was asked to), but embarrassingly stupid in the real world.
Let's look at calories-in vs calories-out in the fixed caloric phase of the Abredeen study.
Calories-in is total calories in to metabolism. There are two sources. Those from the diet, let's assume (incorrectly) these are genuinely all of the 2000kcal/d on offer. Then there is the supply of free fatty acids metered out from adipocytes under the regulation of insulin. Maybe a little glycogen, but I'll ignore that for the discussion.
Under LCHF conditions more FFAs are accessible due to lower insulin levels. More get used and, from Table 1, only 1930kcal of food are needed to supplement those calories-in from adipocytes in order to meet total metabolic needs. Hunger is low. Calories supplied are clearly able to meet voluntary calories out. Demand is within the limits of supply. Some food is refused.
Under MCMF conditions the higher insulin level allows less calories to be supplied from fat in to metabolism (adipose derived calories-in fall), so calories-in accepted from food spontaneously increase to the full 2000kcal/d. Under the study conditions we cannot tell if 2000kcal plus reduced adipose FFA supply is enough for as much metabolic activity as was possible under low insulin conditions. What if it is not? Now the real question is: Does lipolysis automatically increase to supply all needs for calories out? Why should it? Lipolysis is controlled by insulin. Insulin is high, lipolysis restrained.
If there is any shortfall in the calories from fat plus 2000kcal, there are only limited calories available to burn. You can't burn what you don't have. Calories-out would drop because they simply cannot exceed the supply available. I would expect the participants to automatically reduce their calories-out. There is no free lunch. Calories-out = calories-in. All need to be accounted for.
Is it be possible to force lipolysis in the face of hyperinsulinaemia to increase FFAs from fat to a higher level without lowering insulin?
Of course it is. There are other hormones in addition to insulin. You can throw around adrenaline, growth hormone, glucagon and probably a truckload of others I've not thought about. You can add in direct sympathetic nervous system innervation of adipocytes to effect lipolysis if you like. But these mechanisms come with a price. The price is hunger.
I think it's called working up an appetite.
In the Aberdeen study the attempt to maintain caloric intake failed during the LCHF phase because low insulin increased caloric supply from fat. Higher insulin in the MCMF phase limited calories-in derived from adipose tissue and may well have set a cap on total calories available for use during this higher insulin phase.
In Frank's thought experiment it might be easy to fix dietary calories-in, but people might refuse some of them if insulin was low enough for adipose tissue derived FFAs to be available.... If they ate all of their calories but wriggled in their chair a bit more because they had more calories available then the concept of calories-out being fixed is lost....
I'll just finish with a clarification of this phrase from another commenter:
"lipolysis is not beta oxidation"
This is, ultimately, accurate. That doesn't stop it being bollocks.
A rather more perceptive view is the situation comes from, of all places, the lipophobic cardiologists who published on FFAs and myocardial ischaemia:
"The rate of fatty-acid uptake and oxidation by the heart is controlled by their availability [33]"
Oh, interesting. Availability. A supply led system. Hmmmmmm. I would guess most FFA burning tissue would follow cardiac muscle. Now I can't quite remember what effect insulin has on lipolysis and FFA availability. Silly me.
Peter
Frank said...
Hi Peter. I'd say that I pretty much agree with your post. Insulin and caloric deficit are not mutually exclusive, ie, low-insulin could enhance fat loss on a caloric deficit or, looked from another perspective, a caloric deficit could enhance fat loss if someone has low insulin level. I have only one question for you. For the sake of it lets make thing black and white. What do you believe is the most important thing to do, in order to achieve weight/fat loss a) be in a caloric deficit (your insulin level does not matter much) b) having a low-insulin level (it does not matter much if you're in a caloric deficit or not). Again, in real life, I don't believe they exclude each other, but if you could fix only one to have a weight loss, which one would you fix? Calories or insulin? The way I see it is that, as you stated, insulin inhibits lipolysis, but more lipolysis does not equal more oxidation. It still has to be matched to energy expenditure. In that case, calories would be the most important factor. That's my point of view and it could be wrong. I'm just wondering if you agree to some degree with it, because reading your post, I get the idea that you do. Thanks for your time.
Peter said...
Ah Frank, now there is a question. Without caloric deficit (and I want uncoupling proteins, sleeping metabolic rate, spontaneous movements, etc, etc, etc, everything, accounted for) there will be no weight loss. But, in real life, if I could only alter just one, it would be insulin. I would expect no weight loss but I would expect improved health. What else matters?
There is a flaw in the answer I gave to this question. It's working at the Noddy level of calories-in vs calories-out.
The Noddy approach is perfectly adequate to explain the findings of GnK's paper (PR's weight loss excepted, if she genuinely ate all she was asked to), but embarrassingly stupid in the real world.
Let's look at calories-in vs calories-out in the fixed caloric phase of the Abredeen study.
Calories-in is total calories in to metabolism. There are two sources. Those from the diet, let's assume (incorrectly) these are genuinely all of the 2000kcal/d on offer. Then there is the supply of free fatty acids metered out from adipocytes under the regulation of insulin. Maybe a little glycogen, but I'll ignore that for the discussion.
Under LCHF conditions more FFAs are accessible due to lower insulin levels. More get used and, from Table 1, only 1930kcal of food are needed to supplement those calories-in from adipocytes in order to meet total metabolic needs. Hunger is low. Calories supplied are clearly able to meet voluntary calories out. Demand is within the limits of supply. Some food is refused.
Under MCMF conditions the higher insulin level allows less calories to be supplied from fat in to metabolism (adipose derived calories-in fall), so calories-in accepted from food spontaneously increase to the full 2000kcal/d. Under the study conditions we cannot tell if 2000kcal plus reduced adipose FFA supply is enough for as much metabolic activity as was possible under low insulin conditions. What if it is not? Now the real question is: Does lipolysis automatically increase to supply all needs for calories out? Why should it? Lipolysis is controlled by insulin. Insulin is high, lipolysis restrained.
If there is any shortfall in the calories from fat plus 2000kcal, there are only limited calories available to burn. You can't burn what you don't have. Calories-out would drop because they simply cannot exceed the supply available. I would expect the participants to automatically reduce their calories-out. There is no free lunch. Calories-out = calories-in. All need to be accounted for.
Is it be possible to force lipolysis in the face of hyperinsulinaemia to increase FFAs from fat to a higher level without lowering insulin?
Of course it is. There are other hormones in addition to insulin. You can throw around adrenaline, growth hormone, glucagon and probably a truckload of others I've not thought about. You can add in direct sympathetic nervous system innervation of adipocytes to effect lipolysis if you like. But these mechanisms come with a price. The price is hunger.
I think it's called working up an appetite.
In the Aberdeen study the attempt to maintain caloric intake failed during the LCHF phase because low insulin increased caloric supply from fat. Higher insulin in the MCMF phase limited calories-in derived from adipose tissue and may well have set a cap on total calories available for use during this higher insulin phase.
In Frank's thought experiment it might be easy to fix dietary calories-in, but people might refuse some of them if insulin was low enough for adipose tissue derived FFAs to be available.... If they ate all of their calories but wriggled in their chair a bit more because they had more calories available then the concept of calories-out being fixed is lost....
I'll just finish with a clarification of this phrase from another commenter:
"lipolysis is not beta oxidation"
This is, ultimately, accurate. That doesn't stop it being bollocks.
A rather more perceptive view is the situation comes from, of all places, the lipophobic cardiologists who published on FFAs and myocardial ischaemia:
"The rate of fatty-acid uptake and oxidation by the heart is controlled by their availability [33]"
Oh, interesting. Availability. A supply led system. Hmmmmmm. I would guess most FFA burning tissue would follow cardiac muscle. Now I can't quite remember what effect insulin has on lipolysis and FFA availability. Silly me.
Peter
Thursday, March 24, 2011
Fasting insulin and weight loss
I think that it might be a good idea to state here that I'm a calories-in calories-out sort of a person. Arguing about metabolic advantage is pointless. When a person loses weight they convert tissue to energy, amputations excepted. Where the calories go, whether it is BMR, thermogenesis, glycosuria, increased spontaneous movement, shivering etc, the calories always go somewhere. As far as I am aware no one is suggesting that calories evaporate. Certainly I'm not.
I am on blog as stating that dietary fat, in common with carbohydrate, is stored in the aftermath of a meal. If you did not store your dietary fat it would sit there in your chylomicrons until you were as hyperlipaemic as a diabetic on an ADA approved low fat diet. All fat which is not used for on going metabolism must be stored. It may take a few hours to clear chylomicrons but they do get cleared. Mostly in to adipocytes.
EDIT: There is an update on this post here.
Okay, let's look at the Grey and Kipnis (GnK) 1971 paper.
If you take a human like ET, who is maintaining a bodyweight of 142kg by eating 4,200kcal per day, you can adjust her macronutrient ratio to pretty well whatever you like and she will remain weight stable, provided you insist that she always consumes 4,200kcal/d. Insulin will plummet on a high fat diet and this will release necessary fatty acids from adipocytes. These FFAs, the Spawn of Satan, will be both released and used at an increased rate. But will she lose weight? Of course not. She will just re-pack her adipocytes with the extra fat from her fixed, 4,200kcal, low carbohydrate diet. Many people, myself included, can maintain weight stability on a low carbohydrate diet for years.
There's a nice paper about fat accumulation under low insulin conditions on my hard drive. It happens. I will post about it when I feel like it, it looks interesting.
There was one participant in the GnK study, RP, who refused to comply with the study protocol. That's a 20% non compliance rate. She under ate and lost weight. We get no information about her caloric intake at any stage. We know relatively little about her diet (ie sugar vs starch) before the study. We have no idea what sort of carbohydrate was used in the study diet. The only information we have about which phase of the diet gave the weight loss is this graph:

But we certainly have a failure of compliance in this study where an obese subject refused scheduled food and subsequently lost weight. That's worth remembering.
Now let's look at hypocaloric conditions in the same paper. DB, SM and DM were put on to 1,500kcal/d (Keysian starvation) from 2,200kcal/d, 3600kcal/d or 3,800kcal/d respectively. They, err, lost weight. They lost weight pretty nigh on linearly over 12 weeks whether their fasting insulin was 40microIU/ml or 15microIU/ml, produced by adjustment of their carbohydrate intake from 240g/d, down to zero and back to 240g/d.
NB I am perfectly willing to accept these results as they stand but just as an aside; none of the individual records shows any suggestion of a weight shift related to to glycogen depletion/repletion on these changes in carbohydrate intake. The LC phase included zero carbohydrate. The HC version of 1,500kcal provided 72% of calories as some sort of carbohydrate, ie 240g/d. Maybe even Weight Watchers depletes liver glycogen following an overnight fast... A bit odd but probably irrelevant.
Back to the results. The caloric intake was fixed and low. Fat was stored in the LC/HF group and accessed easily because insulin was low. Under high carbohydrate intake calories were stored mostly as glycogen and glucose was metered out to avoid hypoglycaemia. Any fat lost by the lower-but-not-zero rate of lipolysis under high insulin levels was simply not replaced.
Just eat 1,500kcal/d and you will lose weight. Eat more than 1,500kcal and you're a pig.
The study was designed to get exactly these results.
But, out of only five subjects, one obese person became a food refusenick. Various studies have had similar compliance problems, with obese participants refusing food. Let's look at some of them.
I knew there had been a paper by Krauss looking at lipoprotein subgroups during weight stability on assorted carbohydrate intakes. It didn't measure plasma insulin but, if we accept anything from GnK's work, I think we have to accept that under weight stability we can dial fasting insulin by adjusting carbohydrate intake. At least between 4% and about 72% of calories.
Krauss looked at diets composed of 54%, 39% or 26% of energy from carbohydrate, with a bonus group on 26% carbohydrate and (gasp) 15% of total calories as saturated fat.... These folks were instructed to maintain weight stability. This quote had the LC brigade, myself included, giggling if not rolling around in the aisles.
"Despite our effort to maintain constant weight, the 26%-carbohydrate, low-saturated-fat diet group lost more weight than did the 54%-carbohydrate group during the stable-weight period. There was also a trend for a greater reduction in percentage body fat with the lower-carbohydrate diets (P < 0.02, analysis of variance)."
The numbers are in Table 2.
My browser squishes the table, these are the numbers that matter, simplified. Remember, everyone was supposed to be weight stable:

Some of these numbers made p<0.05 or even <0.02, shrug. What is more interesting is the trend in accidental weight loss. Oh and look, the sat fat group didn't lose the most weight, just the most fat. I like that.
My take home message is that the lower the carbohydrate intake (and it is reasonable to assume the lower the fasting insulin) the harder it is to consume enough calories to maintain the obese state. It's possible, but not easy.
Then there is this study looking at the HPA stress axis under fixed calorie low carbohydrate or medium carbohydrate diet conditions. I'll just look at weight and insulin because the changes in the processing of cortisol are about as lucid as Krauss' early papers on lipoprotein changes due to dietary saturated fat. It seems reasonable to assume things improved on LC, otherwise any deterioration would have been headline news. This is a crossover study, the same people did a month on low carb and a month on medium carb, in random order. This makes the results tables somewhat unintelligible but it still comes close to replication the 1,500ckal section of GnK's paper.
Under weight stable conditions fasting insulin was 16.6microIU/ml on 57% carbohydrate. Under LC (4% carbs) conditions, on a fixed 2000kcal intake insulin dropped to 7.3microIU/ml. Weight loss was 7.2kg in 4 weeks. Eating 2000kcal of which 35% was carbs gave 4.7kg weight loss on a fasting insulin of 9.2microIU/ml. After correction for water shifts under LC there was exactly the fat loss accounted for by a caloric deficit of 66kcal/d. This was, oddly enough, exactly the caloric count of the food REFUSED from the 2000kcal provided during the LC phase........... Which they had been asked to eat. Obese people refusing part of a 2000kcal ration.
These folks where in a residential diet study. They consistently refused food they had agreed to eat during the "fixed" caloric intake phase, but only if the macronutrient ratio lowered insulin. As an aside the insulin level on LC was statistically significantly lower than on weight stability but the drop on medium carbohydrate was not. I would argue that the difference between either 7.3microIU/ml or 16.6microIU/ml and 9.2 microIU/ml is biologically significant even if p is > 0.05.
The original report details the menus and a battery of psychological test. There is a mass of information in this study from Aberdeen. As we all know, people mostly seem to get depressed and stoopid on LC diets. In this instance they just stopped being hungry!
Here is one of the best quotes, from the results section:
"The 3-d maintenance diet was designed to 1) neutralize the ketogenic state and replete liver carbohydrate stores and 2) to return hunger to baseline levels— equivalent to the maintenance period 1, before ad libitum feeding—recognizing that a carryover effect from the weight-loss phase existed. This design is particularly relevant for the subjects who were given the LC ketogenic diet first and then the MC nonketogenic diet."
"to return hunger to baseline levels......" I like that. Hunger on the ketogenic diet is not at baseline levels, it is lower. Just supplying MORE calories INCREASES hunger, so long as the calories have carbohydrate at 57%. Hungry and weight stable or less hungry while losing weight. I really like that.
Then a brief quote from this paper, also a weight loss rather than weight stability study, but the quote is too entertaining to leave out.
Fasting insulin was 11.6microIU/ml and 14.4microIU/ml at 3 and 6 months under ad libitum calories but progressively less stringent carbohydrate restriction. Under rigid calorie restricted low fat eating it was steady around 18microIU/ml.
"Based on dietary records, the reduction in daily caloric intake was similar in the two groups. For the greater weight loss in the very low carbohydrate group to be strictly a result of decreased caloric consumption, they would have had to consume approximately 300 fewer calories/d over the first 3 months relative to the low fat diet group (28). Although the inaccuracy of dietary records for obese individuals is well documented (31, 32), it seems unlikely that a systematic discrepancy of this magnitude occurred between groups of subjects who were comparably overweight."
We know that obese people always under report their caloric intake, just ask any obesity expert. Why on earth should this particular group of obese people consistently over report their caloric intake? That's not what fat people do.
You could rephrase this to speculate that the LC group either ate and "used" an extra 300kcal/d or became pathological liars who exaggerated their food intake by 300kcal/d, presumably to wind up the experimenters. Ketosis does make you stoopid and depressed, why shouldn't it make you in to a practical joker too?
Is anyone seeing a pattern of people (or rats) refusing food under reduced insulin conditions?
In the real world people eat when they are hungry, because they are hungry. They don't drink fixed caloric intakes of mysterious liquid formulations from researchers who's rat models are based on either sucrose or vegetable oil.
Can people actually gain weight on high fat diets? Of course they can. You can accumulate fat without elevated insulin. But you are much less likely to gain weight if you are not hungry.
I note that Chris Voight was not on a fixed calorie intake and was not hungry while he lost an impressive amount of his excess weight. I think his fasting insulin was low and he was performing lipolysis at an impressive rate.
Let's make this clear. Fasting insulin determines weight loss. The effect is primarily through reduced dietary caloric intake secondary to lipolysis-mediated access to adipose tissue calorie stores.
Overfeeding in excess of preferred calorie intake breaks the system. GnK simply disabled the mechanism of appetite control by fixing caloric intake. Fine to prove a point. It's this sort of research that has got us where we are today.
NB I think this decrease in hunger probably only occurs in obesity. For those of us who have adopted a LC eating pattern without the need for weight loss (and still have little excess fat) there are clearly other factors coming in to play, as there will be when a previously overweight person approaches target/ideal weight, what ever that might be.
Peter
I am on blog as stating that dietary fat, in common with carbohydrate, is stored in the aftermath of a meal. If you did not store your dietary fat it would sit there in your chylomicrons until you were as hyperlipaemic as a diabetic on an ADA approved low fat diet. All fat which is not used for on going metabolism must be stored. It may take a few hours to clear chylomicrons but they do get cleared. Mostly in to adipocytes.
EDIT: There is an update on this post here.
Okay, let's look at the Grey and Kipnis (GnK) 1971 paper.
If you take a human like ET, who is maintaining a bodyweight of 142kg by eating 4,200kcal per day, you can adjust her macronutrient ratio to pretty well whatever you like and she will remain weight stable, provided you insist that she always consumes 4,200kcal/d. Insulin will plummet on a high fat diet and this will release necessary fatty acids from adipocytes. These FFAs, the Spawn of Satan, will be both released and used at an increased rate. But will she lose weight? Of course not. She will just re-pack her adipocytes with the extra fat from her fixed, 4,200kcal, low carbohydrate diet. Many people, myself included, can maintain weight stability on a low carbohydrate diet for years.
There's a nice paper about fat accumulation under low insulin conditions on my hard drive. It happens. I will post about it when I feel like it, it looks interesting.
There was one participant in the GnK study, RP, who refused to comply with the study protocol. That's a 20% non compliance rate. She under ate and lost weight. We get no information about her caloric intake at any stage. We know relatively little about her diet (ie sugar vs starch) before the study. We have no idea what sort of carbohydrate was used in the study diet. The only information we have about which phase of the diet gave the weight loss is this graph:

But we certainly have a failure of compliance in this study where an obese subject refused scheduled food and subsequently lost weight. That's worth remembering.
Now let's look at hypocaloric conditions in the same paper. DB, SM and DM were put on to 1,500kcal/d (Keysian starvation) from 2,200kcal/d, 3600kcal/d or 3,800kcal/d respectively. They, err, lost weight. They lost weight pretty nigh on linearly over 12 weeks whether their fasting insulin was 40microIU/ml or 15microIU/ml, produced by adjustment of their carbohydrate intake from 240g/d, down to zero and back to 240g/d.
NB I am perfectly willing to accept these results as they stand but just as an aside; none of the individual records shows any suggestion of a weight shift related to to glycogen depletion/repletion on these changes in carbohydrate intake. The LC phase included zero carbohydrate. The HC version of 1,500kcal provided 72% of calories as some sort of carbohydrate, ie 240g/d. Maybe even Weight Watchers depletes liver glycogen following an overnight fast... A bit odd but probably irrelevant.
Back to the results. The caloric intake was fixed and low. Fat was stored in the LC/HF group and accessed easily because insulin was low. Under high carbohydrate intake calories were stored mostly as glycogen and glucose was metered out to avoid hypoglycaemia. Any fat lost by the lower-but-not-zero rate of lipolysis under high insulin levels was simply not replaced.
Just eat 1,500kcal/d and you will lose weight. Eat more than 1,500kcal and you're a pig.
The study was designed to get exactly these results.
But, out of only five subjects, one obese person became a food refusenick. Various studies have had similar compliance problems, with obese participants refusing food. Let's look at some of them.
I knew there had been a paper by Krauss looking at lipoprotein subgroups during weight stability on assorted carbohydrate intakes. It didn't measure plasma insulin but, if we accept anything from GnK's work, I think we have to accept that under weight stability we can dial fasting insulin by adjusting carbohydrate intake. At least between 4% and about 72% of calories.
Krauss looked at diets composed of 54%, 39% or 26% of energy from carbohydrate, with a bonus group on 26% carbohydrate and (gasp) 15% of total calories as saturated fat.... These folks were instructed to maintain weight stability. This quote had the LC brigade, myself included, giggling if not rolling around in the aisles.
"Despite our effort to maintain constant weight, the 26%-carbohydrate, low-saturated-fat diet group lost more weight than did the 54%-carbohydrate group during the stable-weight period. There was also a trend for a greater reduction in percentage body fat with the lower-carbohydrate diets (P < 0.02, analysis of variance)."
The numbers are in Table 2.
My browser squishes the table, these are the numbers that matter, simplified. Remember, everyone was supposed to be weight stable:

Some of these numbers made p<0.05 or even <0.02, shrug. What is more interesting is the trend in accidental weight loss. Oh and look, the sat fat group didn't lose the most weight, just the most fat. I like that.
My take home message is that the lower the carbohydrate intake (and it is reasonable to assume the lower the fasting insulin) the harder it is to consume enough calories to maintain the obese state. It's possible, but not easy.
Then there is this study looking at the HPA stress axis under fixed calorie low carbohydrate or medium carbohydrate diet conditions. I'll just look at weight and insulin because the changes in the processing of cortisol are about as lucid as Krauss' early papers on lipoprotein changes due to dietary saturated fat. It seems reasonable to assume things improved on LC, otherwise any deterioration would have been headline news. This is a crossover study, the same people did a month on low carb and a month on medium carb, in random order. This makes the results tables somewhat unintelligible but it still comes close to replication the 1,500ckal section of GnK's paper.
Under weight stable conditions fasting insulin was 16.6microIU/ml on 57% carbohydrate. Under LC (4% carbs) conditions, on a fixed 2000kcal intake insulin dropped to 7.3microIU/ml. Weight loss was 7.2kg in 4 weeks. Eating 2000kcal of which 35% was carbs gave 4.7kg weight loss on a fasting insulin of 9.2microIU/ml. After correction for water shifts under LC there was exactly the fat loss accounted for by a caloric deficit of 66kcal/d. This was, oddly enough, exactly the caloric count of the food REFUSED from the 2000kcal provided during the LC phase........... Which they had been asked to eat. Obese people refusing part of a 2000kcal ration.
These folks where in a residential diet study. They consistently refused food they had agreed to eat during the "fixed" caloric intake phase, but only if the macronutrient ratio lowered insulin. As an aside the insulin level on LC was statistically significantly lower than on weight stability but the drop on medium carbohydrate was not. I would argue that the difference between either 7.3microIU/ml or 16.6microIU/ml and 9.2 microIU/ml is biologically significant even if p is > 0.05.
The original report details the menus and a battery of psychological test. There is a mass of information in this study from Aberdeen. As we all know, people mostly seem to get depressed and stoopid on LC diets. In this instance they just stopped being hungry!
Here is one of the best quotes, from the results section:
"The 3-d maintenance diet was designed to 1) neutralize the ketogenic state and replete liver carbohydrate stores and 2) to return hunger to baseline levels— equivalent to the maintenance period 1, before ad libitum feeding—recognizing that a carryover effect from the weight-loss phase existed. This design is particularly relevant for the subjects who were given the LC ketogenic diet first and then the MC nonketogenic diet."
"to return hunger to baseline levels......" I like that. Hunger on the ketogenic diet is not at baseline levels, it is lower. Just supplying MORE calories INCREASES hunger, so long as the calories have carbohydrate at 57%. Hungry and weight stable or less hungry while losing weight. I really like that.
Then a brief quote from this paper, also a weight loss rather than weight stability study, but the quote is too entertaining to leave out.
Fasting insulin was 11.6microIU/ml and 14.4microIU/ml at 3 and 6 months under ad libitum calories but progressively less stringent carbohydrate restriction. Under rigid calorie restricted low fat eating it was steady around 18microIU/ml.
"Based on dietary records, the reduction in daily caloric intake was similar in the two groups. For the greater weight loss in the very low carbohydrate group to be strictly a result of decreased caloric consumption, they would have had to consume approximately 300 fewer calories/d over the first 3 months relative to the low fat diet group (28). Although the inaccuracy of dietary records for obese individuals is well documented (31, 32), it seems unlikely that a systematic discrepancy of this magnitude occurred between groups of subjects who were comparably overweight."
We know that obese people always under report their caloric intake, just ask any obesity expert. Why on earth should this particular group of obese people consistently over report their caloric intake? That's not what fat people do.
You could rephrase this to speculate that the LC group either ate and "used" an extra 300kcal/d or became pathological liars who exaggerated their food intake by 300kcal/d, presumably to wind up the experimenters. Ketosis does make you stoopid and depressed, why shouldn't it make you in to a practical joker too?
Is anyone seeing a pattern of people (or rats) refusing food under reduced insulin conditions?
In the real world people eat when they are hungry, because they are hungry. They don't drink fixed caloric intakes of mysterious liquid formulations from researchers who's rat models are based on either sucrose or vegetable oil.
Can people actually gain weight on high fat diets? Of course they can. You can accumulate fat without elevated insulin. But you are much less likely to gain weight if you are not hungry.
I note that Chris Voight was not on a fixed calorie intake and was not hungry while he lost an impressive amount of his excess weight. I think his fasting insulin was low and he was performing lipolysis at an impressive rate.
Let's make this clear. Fasting insulin determines weight loss. The effect is primarily through reduced dietary caloric intake secondary to lipolysis-mediated access to adipose tissue calorie stores.
Overfeeding in excess of preferred calorie intake breaks the system. GnK simply disabled the mechanism of appetite control by fixing caloric intake. Fine to prove a point. It's this sort of research that has got us where we are today.
NB I think this decrease in hunger probably only occurs in obesity. For those of us who have adopted a LC eating pattern without the need for weight loss (and still have little excess fat) there are clearly other factors coming in to play, as there will be when a previously overweight person approaches target/ideal weight, what ever that might be.
Peter
Saturday, March 19, 2011
Gourmand Rats?
You know how it is when CarbSane quotes a paper which refutes the carbohydrate hypothesis of obesity. You really can't be *rsed to chase it but you also know that there will be a fundamentally flawed approach which needs looking at. CarbSane was my route in to Kathleen Axen's work with transfats, which I've probably not finished with yet, but which markedly ramped up my dislike of these industrial lipotoxins. I really enjoyed digging back through the Axen papers, though it took hours, and there's no way I would have hit on them without CarbSane's dire (and incorrect) opinion of LC eating based on the last of the triad. Cracking.
So it is with Grey and Kipnis' paper on the irrelevance of fasting insulin to weight loss. It leads back to a rat paper (aren't you surprised!). The rat model was developed to allow rats to gain weight under hypoinsulinaemic conditions. So GnK had a high carbohydrate diet and a low carbohydrate diet for their rats, both of which promoted weight gain, but the LC diet did it without raised insulin. Here are the diets:

Nice.
But here's the funny part. They did a whole load of experiments (very interesting, seminal work on pancreatic glucokinase induction/suppression) which required equal calorie intake between a group on the high carbohydrate diet and another group on the zero carbohydrate diet. Let me quote:
"Since the low carbohydrate-high fat diet is less palatable to rats than the high carbohydrate diet, pair feeding was accomplished by determining the caloric intake of the low carbohydrate fed rats and then offering a comparable [ie less than they would have eaten] caloric amount of the high carbohydrate diet the following day to another group of animals."
You just have to admire the palate of those hypoinsulinaemic rats. Of course it's just possible they weren't ratty gourmands, it might actually be that they just weren't hungry because their fasting insulin was low and no one was ordering them to eat more than they felt like................
The giggles that come from following CarbSane's leads! Gotta get them from somewhere.
More on the cited Grey and Kipins 1971 paper when I've finished with the modern studies looking at the same question. There are some nice ones.
Peter
Tuesday, March 15, 2011
Cholesterol and cholestyramine
I'm not ready to post about this study yet but I thought I'd just put up a flag for its existence. It has long puzzled me why cholestryamine should show any benefit in cardiovascular disease, even if any benefit is offset by increased non cardiovascular mortality.
It turns out that cholestyramine increases the blood level of at least one oxysterol 25 fold. I would guess that this is accumulated in Lp(a).
This is of particular interest to me. I'll get around to why one day but thanks to Leib at THINCS for the lead in to the whole area.
So cholestyramine: When you look at all of the metabolic benefits which come with this wonder drug it's just amazing it doesn't save any lives.

Could it be that the multiple metabolic benefits (or the accumulated oxysterols, gasp, heresy again) reduce cvd mortality while the low cholesterol encourages you to throw a punch in some bar in down town Dallas?
Peter
It turns out that cholestyramine increases the blood level of at least one oxysterol 25 fold. I would guess that this is accumulated in Lp(a).
This is of particular interest to me. I'll get around to why one day but thanks to Leib at THINCS for the lead in to the whole area.
So cholestyramine: When you look at all of the metabolic benefits which come with this wonder drug it's just amazing it doesn't save any lives.

Could it be that the multiple metabolic benefits (or the accumulated oxysterols, gasp, heresy again) reduce cvd mortality while the low cholesterol encourages you to throw a punch in some bar in down town Dallas?
Peter
Spawn of Satan in the gym
I think it's pretty well established that free fatty acids are the Spawn of Satan.
This paper came my way through Luca and THINCS. Free fatty acids are just appalling. Read this paragraph from the discussion section and clutch at your chest:
"... studies have shown that a fat-enriched meal, in contrast to a high carbohydrate meal (HCM), is associated with endothelial activation [30] and may initiate injury to the blood vessel wall [31]. Increased circulating FFA and their derivatives have also been shown to be particularly deleterious on myocardial function during ischemia and reperfusion (for review see Ref. [32]). Indeed, in the ischemic myocardium, long-chain fatty acids accumulate quickly. The rate of fatty-acid uptake and oxidation by the heart is controlled by their availability [33]. Exogenous fatty acids, the main metabolic fuel of the myocardium under aerobic conditions, are detrimental during oxygen deprivation since their presence further augments the accumulation of long-chain acyl esters in the myocytes. The accumulation of lipids and their degradation products may contribute to the progression of injury. Furthermore, during reperfusion, fatty-acid oxidation can quickly recover and become the dominant source of ATP production. A high rate of fatty-acid oxidation contributes to a marked decrease in cardiac efficiency during the ischemia–reperfusion period [34]. We have previously shown that pharmacologically-induced increase in plasma FFA can significantly reduce the ischemic threshold in patients with stable coronary artery disease [35]. Recent studies have shown that FFA may also attenuate endothelium-dependent arterial vasodilatation [17,36] and increase sympathetic drive and alpha 1-adrenergic receptor reactivity and tone [37]. In addition, a HFM leads to an increase in calf vascular resistance [38]. All these data support a role for FFA and triglycerides both in vascular and muscular metabolic regulations."
I have to say that I've been through most of the references cited and many of them are quite hysterical. But that's another matter, maybe another post.
So the people who wrote the above paragraph had the bravery to feed a high fat meal, a high carbohydrate meal or nothing (on different days) to some cardiac patients and then treadmilled them to ST segment depression, ie until myocardial ischaemia set in. Obviously a high fat meal, particularly one based on saturated fat (as the test meal is claimed to have been, you don't get enough detail to tell what they used) should have crippled these people.
It didn't. The high fat meal had absolutely no effect on time to ischaemia.
How do they explain this? Easy, the high fat meal may have been a high fat meal, but it never raised plasma free fatty acids! This is what they say:
"However, this study was targeted to assess the role of a high fat meal and not of high serum FFA concentration; in fact due to the antilypolitic effect of the hyperinsulinemic response to the meal the serum FFA concentration was lower than in the fasting state."
Cunning hey? Just spike the high fat meal with exactly the correct amount of carbohydrate to lower lipolysis derived FFAs by an amount slightly more than the test meal generates and there is no overall change in FFAs (p > 0.05, ns) so no change in time to ischaemia! Beautifully done. But bollocks never the less.
Aside: Weird how you can use insulin to inhibit lipolysis in heart patients, just like treating ketoacidosis. You might almost imagine that insulin has something to do with weight control, I dunno... Back to the bollocks:
The same number of calories consumed as mostly carbohydrate dropped the time to ischaemia from 376 seconds to 297 seconds, p = 0.003, Table 2, line 13. This is despite the fact that carbohydrate meal reduced the Spawn of Satan from 0.89mmol/l to 0.27mmol/l, p = 0.002.

Of course with all that hard evidence about FFAs delaying myocardial recovery you really would expect an accelerated recovery from ST segment depression after the high carbohydrate meal, after all FFAs concentration is only a third of that under fasting conditions. In fact we can see from line 15 that the high carbohydrate meal gave a recovery time 30 seconds slower than after fasting, with all of that Spawn of Satan released from adipocytes due to not eating for a few hours. The high fat meal gave a recovery time which was 30 second faster. The spread in the numbers means that all of these differences are ns. No way can we tell how close p got to that good old 0.05, ns is all we get. But you really do have to wonder about how this fits in with all of those references in the above quote!
These authors do not go so far as to make dietary recommendations for folks with cardiovascular disease eager to spend a few minutes on a treadmill after supper.
Cardiologists back in the 1990s were not so reticent. This paper came out in 1996. It is essentially a poor man's version of the modern epic discussed above, with identical findings. What is the dietary advice if you have angina in Sheffield in 1996? Eat fat or carbohydrate before your jogging?
"It would be difficult to advise patients to take a higher proportion of calories as fat in the diet to minimize these early adverse cardiovascular effects, because of the potential effects of dietary fat on atherosclerosis genesis."
And the solution, just say no!
"...patients with angina should be advised to limit their activities in the early (first 30 min) postprandial period because of the reduction in angina threshold."
So if you are planning some post prandial exercise you can have an extra 79 seconds before myocardial ischaemic sets in by having cream instead of potatoes, but don't. Instead just put your feet up!
Peter
This paper came my way through Luca and THINCS. Free fatty acids are just appalling. Read this paragraph from the discussion section and clutch at your chest:
"... studies have shown that a fat-enriched meal, in contrast to a high carbohydrate meal (HCM), is associated with endothelial activation [30] and may initiate injury to the blood vessel wall [31]. Increased circulating FFA and their derivatives have also been shown to be particularly deleterious on myocardial function during ischemia and reperfusion (for review see Ref. [32]). Indeed, in the ischemic myocardium, long-chain fatty acids accumulate quickly. The rate of fatty-acid uptake and oxidation by the heart is controlled by their availability [33]. Exogenous fatty acids, the main metabolic fuel of the myocardium under aerobic conditions, are detrimental during oxygen deprivation since their presence further augments the accumulation of long-chain acyl esters in the myocytes. The accumulation of lipids and their degradation products may contribute to the progression of injury. Furthermore, during reperfusion, fatty-acid oxidation can quickly recover and become the dominant source of ATP production. A high rate of fatty-acid oxidation contributes to a marked decrease in cardiac efficiency during the ischemia–reperfusion period [34]. We have previously shown that pharmacologically-induced increase in plasma FFA can significantly reduce the ischemic threshold in patients with stable coronary artery disease [35]. Recent studies have shown that FFA may also attenuate endothelium-dependent arterial vasodilatation [17,36] and increase sympathetic drive and alpha 1-adrenergic receptor reactivity and tone [37]. In addition, a HFM leads to an increase in calf vascular resistance [38]. All these data support a role for FFA and triglycerides both in vascular and muscular metabolic regulations."
I have to say that I've been through most of the references cited and many of them are quite hysterical. But that's another matter, maybe another post.
So the people who wrote the above paragraph had the bravery to feed a high fat meal, a high carbohydrate meal or nothing (on different days) to some cardiac patients and then treadmilled them to ST segment depression, ie until myocardial ischaemia set in. Obviously a high fat meal, particularly one based on saturated fat (as the test meal is claimed to have been, you don't get enough detail to tell what they used) should have crippled these people.
It didn't. The high fat meal had absolutely no effect on time to ischaemia.
How do they explain this? Easy, the high fat meal may have been a high fat meal, but it never raised plasma free fatty acids! This is what they say:
"However, this study was targeted to assess the role of a high fat meal and not of high serum FFA concentration; in fact due to the antilypolitic effect of the hyperinsulinemic response to the meal the serum FFA concentration was lower than in the fasting state."
Cunning hey? Just spike the high fat meal with exactly the correct amount of carbohydrate to lower lipolysis derived FFAs by an amount slightly more than the test meal generates and there is no overall change in FFAs (p > 0.05, ns) so no change in time to ischaemia! Beautifully done. But bollocks never the less.
Aside: Weird how you can use insulin to inhibit lipolysis in heart patients, just like treating ketoacidosis. You might almost imagine that insulin has something to do with weight control, I dunno... Back to the bollocks:
The same number of calories consumed as mostly carbohydrate dropped the time to ischaemia from 376 seconds to 297 seconds, p = 0.003, Table 2, line 13. This is despite the fact that carbohydrate meal reduced the Spawn of Satan from 0.89mmol/l to 0.27mmol/l, p = 0.002.

Of course with all that hard evidence about FFAs delaying myocardial recovery you really would expect an accelerated recovery from ST segment depression after the high carbohydrate meal, after all FFAs concentration is only a third of that under fasting conditions. In fact we can see from line 15 that the high carbohydrate meal gave a recovery time 30 seconds slower than after fasting, with all of that Spawn of Satan released from adipocytes due to not eating for a few hours. The high fat meal gave a recovery time which was 30 second faster. The spread in the numbers means that all of these differences are ns. No way can we tell how close p got to that good old 0.05, ns is all we get. But you really do have to wonder about how this fits in with all of those references in the above quote!
These authors do not go so far as to make dietary recommendations for folks with cardiovascular disease eager to spend a few minutes on a treadmill after supper.
Cardiologists back in the 1990s were not so reticent. This paper came out in 1996. It is essentially a poor man's version of the modern epic discussed above, with identical findings. What is the dietary advice if you have angina in Sheffield in 1996? Eat fat or carbohydrate before your jogging?
"It would be difficult to advise patients to take a higher proportion of calories as fat in the diet to minimize these early adverse cardiovascular effects, because of the potential effects of dietary fat on atherosclerosis genesis."
And the solution, just say no!
"...patients with angina should be advised to limit their activities in the early (first 30 min) postprandial period because of the reduction in angina threshold."
So if you are planning some post prandial exercise you can have an extra 79 seconds before myocardial ischaemic sets in by having cream instead of potatoes, but don't. Instead just put your feet up!
Peter
Sunday, March 06, 2011
Potatoes and weight loss (1)
I tried and failed to produce a comprehensive post about weight loss on an all potato diet. It runs to too many pages. This is a brief simplification.
Eating 2-3000kcal/day of potatoes spikes blood glucose. The more potatoes you eat the more you spike glucose. The pancreas responds to hyperglycaemia by secreting insulin but also by upregulating pancreatic glucokinase production, which increases insulin secretion per unit rise in glucose. After a couple of days on an all potato diet your pancreas will be producing impressive amounts of post prandial insulin.
Adipocytes respond to the insulin by shutting down lipolysis. Plasma free fatty acids drop and fat loss stops.
Insulin is degraded by insulin degrading enzyme. Very, very, very crudely (with a ton of qualifications, read the paper!) insulin action leads to insulin degradation. All insulin sensitive tissues degrade insulin. The liver is a massive sink for insulin, especially on a high carbohydrate diet. Anything which increases hepatic insulin sensitivity should increase hepatic insulin degradation. A sudden ceasation of free fatty acid supply from adipocytes will increase both hepatic insulin sensitivity and hepatic insulin degradation. A potato diet supplies relatively little in the way of fatty acids so there is also little dietary fat to supply the lipid intermediates to encourage hepatic insulin resistance.
Much of the hepatic uptake of glucose occurs without the direct intervention of insulin. The liver has large numbers of GLUT2s on its cells, which allow insulin-independent hepatic glucose uptake via a simple concentration gradient. The gradient is maintained by the intracellular phosphorylation of glucose, which allows its prompt removal to metabolism or storage as glycogen. Hepatic glucokinase does this phosphorylation and the production of the glucokinase enzyme in the liver is, of course, controlled by insulin. Increased insulin leads to increased glucokinase production and enhanced GLUT2 mediated glucose uptake.
Without fat, bulk calories are stored as glycogen, excepting that there is a little de novo fat synthesis from glucose in the liver. Hepatic glycogen does not cause hepatic insulin resistance. In the near absence of FFA supply the liver maintains insulin sensitivity and the ability to degrade insulin. Nothing like as much insulin reaches the periphery as is produced by the pancreas in response to 2-3000kcal of potatoes.
The second effect of shutting down free fatty acid supply from adipocytes and diet is the loss of fatty acid intermediates in muscle. Insulin sensitivity increases, the amount of insulin needed to facilitate glucose uptake by muscles decreases. Insulin secretion from the pancreas will then decrease but hepatic extraction of insulin continues while ever carbohydrate adaption continues.
The ultimate determinant of weight loss is fasting insulin. This determines how much lipolysis occurs during the period before the next meal. No one expects to lose weight during the 4 hours immediately after any meal. The following 8 hours, especially overnight, is when weight loss occurs.
Post absorptively, without dietary glucose input, there is no stimulus for anything other than basal insulin secretion. Fasting insulin will be low because muscles are insulin sensitive so relatively little insulin is needed for glucose uptake. As fasting insulin levels drop lipolysis will restart. Free fatty acids will feed back to the liver to cause some degree of hepatic insulin resistance, decrease first pass metabolism and stop too profound an hypoinsulinaemia occurring. But fat loss will happen.
So you have to ask whether an almost all potato diet genuinely leads low fasting insulin and subsequent weight loss. For my perspective the answer is yes. The precedent for this has to the Kitavans with fasting insulin levels of 4.0microIU/ml.
The next question is whether anyone could do this. That, I suspect, depends on how broken your liver is, ie is there irreversible hepatic insulin resistance. If you are overweight secondary to simple fatty liver, which is completely reversible, I suspect the answer is yes. If you have pathology in your liver such as NASH, especially with fibrosis, I think you might not respond in the same way. The more of a problem you have with obesity the less likely you are to lose weight or experience appetite normalisation (translates as access to adipose tissue calories). Ultimately the ability to live on varied macronutrient ratios comes down to how broken you are, especially your liver. Why a broken liver requires low carbohydrate eating is another post.
Is it healthy for someone with a functional liver to live on potatoes? It is clearly possible in the medium term. Cooked tubers have a respectable history of human usage. If you are not broken it might be a reasonable diet. There are no trans fats in spuds. There are minimal omega 6 fats. There is no gluten. There is just enough fructose to activate hepatic glucokinase without generating de novo lipogenesis. There is adequate high quality protein. On the down side there are a stack of vitamin and mineral deficiencies waiting in the wings.
I have no doubt that Chris Voight lost weight on an all potato diet. I also have no doubt that he was neither chronically hyperglycaemic nor hyperinsulinaemic.
There is no way of putting numbers to the framework with the data I have at the moment, but the physiology is comprehensible.
OK, up for shredding.
Peter
There are a whole stack of follow on posts to this one but let's see how this one holds up first...
Eating 2-3000kcal/day of potatoes spikes blood glucose. The more potatoes you eat the more you spike glucose. The pancreas responds to hyperglycaemia by secreting insulin but also by upregulating pancreatic glucokinase production, which increases insulin secretion per unit rise in glucose. After a couple of days on an all potato diet your pancreas will be producing impressive amounts of post prandial insulin.
Adipocytes respond to the insulin by shutting down lipolysis. Plasma free fatty acids drop and fat loss stops.
Insulin is degraded by insulin degrading enzyme. Very, very, very crudely (with a ton of qualifications, read the paper!) insulin action leads to insulin degradation. All insulin sensitive tissues degrade insulin. The liver is a massive sink for insulin, especially on a high carbohydrate diet. Anything which increases hepatic insulin sensitivity should increase hepatic insulin degradation. A sudden ceasation of free fatty acid supply from adipocytes will increase both hepatic insulin sensitivity and hepatic insulin degradation. A potato diet supplies relatively little in the way of fatty acids so there is also little dietary fat to supply the lipid intermediates to encourage hepatic insulin resistance.
Much of the hepatic uptake of glucose occurs without the direct intervention of insulin. The liver has large numbers of GLUT2s on its cells, which allow insulin-independent hepatic glucose uptake via a simple concentration gradient. The gradient is maintained by the intracellular phosphorylation of glucose, which allows its prompt removal to metabolism or storage as glycogen. Hepatic glucokinase does this phosphorylation and the production of the glucokinase enzyme in the liver is, of course, controlled by insulin. Increased insulin leads to increased glucokinase production and enhanced GLUT2 mediated glucose uptake.
Without fat, bulk calories are stored as glycogen, excepting that there is a little de novo fat synthesis from glucose in the liver. Hepatic glycogen does not cause hepatic insulin resistance. In the near absence of FFA supply the liver maintains insulin sensitivity and the ability to degrade insulin. Nothing like as much insulin reaches the periphery as is produced by the pancreas in response to 2-3000kcal of potatoes.
The second effect of shutting down free fatty acid supply from adipocytes and diet is the loss of fatty acid intermediates in muscle. Insulin sensitivity increases, the amount of insulin needed to facilitate glucose uptake by muscles decreases. Insulin secretion from the pancreas will then decrease but hepatic extraction of insulin continues while ever carbohydrate adaption continues.
The ultimate determinant of weight loss is fasting insulin. This determines how much lipolysis occurs during the period before the next meal. No one expects to lose weight during the 4 hours immediately after any meal. The following 8 hours, especially overnight, is when weight loss occurs.
Post absorptively, without dietary glucose input, there is no stimulus for anything other than basal insulin secretion. Fasting insulin will be low because muscles are insulin sensitive so relatively little insulin is needed for glucose uptake. As fasting insulin levels drop lipolysis will restart. Free fatty acids will feed back to the liver to cause some degree of hepatic insulin resistance, decrease first pass metabolism and stop too profound an hypoinsulinaemia occurring. But fat loss will happen.
So you have to ask whether an almost all potato diet genuinely leads low fasting insulin and subsequent weight loss. For my perspective the answer is yes. The precedent for this has to the Kitavans with fasting insulin levels of 4.0microIU/ml.
The next question is whether anyone could do this. That, I suspect, depends on how broken your liver is, ie is there irreversible hepatic insulin resistance. If you are overweight secondary to simple fatty liver, which is completely reversible, I suspect the answer is yes. If you have pathology in your liver such as NASH, especially with fibrosis, I think you might not respond in the same way. The more of a problem you have with obesity the less likely you are to lose weight or experience appetite normalisation (translates as access to adipose tissue calories). Ultimately the ability to live on varied macronutrient ratios comes down to how broken you are, especially your liver. Why a broken liver requires low carbohydrate eating is another post.
Is it healthy for someone with a functional liver to live on potatoes? It is clearly possible in the medium term. Cooked tubers have a respectable history of human usage. If you are not broken it might be a reasonable diet. There are no trans fats in spuds. There are minimal omega 6 fats. There is no gluten. There is just enough fructose to activate hepatic glucokinase without generating de novo lipogenesis. There is adequate high quality protein. On the down side there are a stack of vitamin and mineral deficiencies waiting in the wings.
I have no doubt that Chris Voight lost weight on an all potato diet. I also have no doubt that he was neither chronically hyperglycaemic nor hyperinsulinaemic.
There is no way of putting numbers to the framework with the data I have at the moment, but the physiology is comprehensible.
OK, up for shredding.
Peter
There are a whole stack of follow on posts to this one but let's see how this one holds up first...
Tuesday, March 01, 2011
Ratty at a year
Ratty, about a year old, 410gm. Ad lib high fat diet, mostly portions of our food. Lots of lard, probably not diabetic! He is very, very strong for his size and can open the cage door after I bent the door clip tighter. Now he sleeps in rat Alcatraz overnight.

Peter
Oh, and here he is with Ping in the background...


Peter
Oh, and here he is with Ping in the background...

Monday, February 28, 2011
Peter eats vegetables

Vegicide at home. And there's a mushroom under the round of goat's cheese... I do this sort of thing occasionally.
Peter
Monday, February 21, 2011
The 14.4% solution

Ok, Ratty, myself and family really are doomed. Again.
How many times does this have to happen before I really start peeing glucose down the loo?
Here's the abstract:
OK, finished that? Clever stuff. Are you scared of a ketogenic diet? Want to pay for the full text to see how I'm going to get diabetes? Don't bother, Emily that nice psychiatrist at Evolutionary Psychiatry has already sent me the pdf. This is what it will take you 30 seconds to locate:
And this is the discussion on the relevant lipotoxin, with my translations in italics:
The present study used hydrogenated corn oil for dietary fat sources since it has less harmful effect on diabetes than lard, even though it contained trans fat.27
Translation: This study did not use hydrogenated corn oil. It used PARTIALLY hydrogenated corn oil, full hydrogenation would eliminate all trans fats. Bollocks statement number two is that trans fats have a less harmful effect on diabetes than lard. Ref 27 is an opinion piece/review by Walter Willett and friends. They suggest "Consumption of partially hydrogenated fats should be minimized". Correct. Willett's weird ideas on saturated fats are as well known as they are incorrect. There is no suggestion in the abstract of the cited review that trans fats are less diabetogenic than lard. Anyone can slog through the free full text to see if there is any justification for the beneficial effects of trans fats vs lard. I can't be @rsed.
The role of trans fat in the development of type 2 diabetes has not been as widely investigated.
Translation: Kathleen Axen beat us to this in 2003 but we're not going to mention someone who is that far ahead of us.
EDIT: Perhaps these jokers only read the abstract of the study in which Kathleen Axen was so limited on word count that any mention of trans fats was omitted from the said abstract. Perhaps Park et al only read the abstract and missed the fact that they had been pre empted by eight years on the glucose dysregulation effects of trans fats. Sigh, the penalty of tight word counts.... Back to translating the discussion. END EDIT
The Nurses’ Health Study,28 the largest and most detailed epidemiological study, showed a positive association between trans fat intake and risk of diabetes, with a clear dose–response relation.
Translation: The NHS is observational and suggests the hypothesis that diabetes is caused by trans fats in a dose related manner. Probably true but needs testing.
However, small epidemiological studies or those that did not include repeated measures of diet did not indicate a positive association.29
Translation: Small, third rate studies are small, third rate studies. We'll cite them because we want to to use trans fats to produce pathology and blame it on the ketogenic nature of our experimental diet.
Tardy et al.30 showed that it [trans fat] does not seem to impair insulin sensitivity, at least in the muscle of rats.
Translation: The site of trans fat toxicity is not muscle. And so???? What about the liver, central to diabetes?
KTD [as used in the current study] did not reverse, but rather exacerbated, the effects of pancreatectomy-induced diabetes. Thus, hydrogenated corn oil was used as a dietary fat instead of lard.
Translation: We're idiots
And from the summary, the last sentence of the paper:
Therefore, KTD, but not ketone, exacerbates impaired energy and glucose metabolism in type 2 diabetic rats, suggesting that it may not be an appropriate dietary intervention for non-obese type 2 diabetic patients.
Translation: A ketogenic diet based on 14.4% of dietary fat in the form of trans fats will make you ill. Very ill. WE'RE IDIOTS.
TRANS FATS: JUST SAY NO.
JUST SAY NO
NO.
Peter
Sunday, February 13, 2011
Dr Wolfgang Lutz Obituary
I've been off the net for so long I've no idea whether this is common knowledge. Dr Lutz was a core influence on me. His writing is so down to earth, pragmatic, sensible and thought provoking. I don't know what else to say.
Peter
Peter
Saturday, February 12, 2011
Normoglycaemia independent of insulin?
This post has been lying around for a while so I'll just stick it up before getting on to IDE and potatoes.
You sometimes have interesting conversations in reception. A lady commented to me that she had no trouble getting arthritis meds in to her dog, some difficulty with antibiotics and that there was no way that she could persuade him to take the tramadol which had been prescribed as a supplementary analgesic for his arthritis.
I mentioned that he might not find the psychotropic effects of tramadol pleasant. A bit like morphine, not everyone finds the effects enjoyable. She concurred about the effects of morphine. It turned out that she had once been given morphine after surgery and had lost her automatic ability to breathe.... A sort of iatrogenic and thankfully temporary Ondine's curse. More poetically here.
In her case the solution had been that a nurse was assigned to sit by her bed and remind her to take a breath whenever she forgot, until automaticity of breathing returned as the morphine wore off. It's a rare side effect.
It started me thinking about control systems. The pancreas monitors blood glucose and responds with insulin and glucagon. It has a generous nerve supply with a whole host of neurotransmitters affecting insulin output. There are also glucoreceptors in the aortic bodies feeding information to the autonomic nervous system. There are, not surprisingly, nuclei in the brain which have glucosensors. There are probably insulin receptors in the brain too.
I think it is just worth pointing out that I have absolutely no problem with the fact that the brain controls blood glucose. Not the pancreas, not the liver, not the adipocytes. Long term stability needs brain input. You could probably say the same about body weight.
It's an integrated system.
But I doubt very much that the brain is central to the bulk management of metabolism. You would hardly expect a regulatory system such as the pancreas/liver/glucose axis to be intrinsically unstable and only kept functional by continuous and aggressive brain intervention. Metabolism ought to be largely self regulatory, with fine tuning by the brain to meet specific conditions.
Aside: Apparently the Eurofighter is intrinsically unstable in flight and is kept stable by enormous computing power and continuous hardware activity. It uses this intrinsic instability, given tightly controlled expression, in order to flip the aircraft from zero to 7 G in a completely unreasonable period of time. Keeping the pilot conscious under these conditions is the challenge to be met. I only heard any of this because we had an interesting presentation about this latter aspect at an anaesthesia meeting on cerebral perfusion pressures not so long back... Back to metabolism:
There is clearly a regulatory set point for the control of breathing. There is also one for blood pressure, blood sodium, potassium, pretty well everything else. I manipulate many of these daily to earn a living. Why not one for bodyweight?
At the moment I have an insulinocentric view of metabolism and bodyweight. Insulin appears to explain a fairly large chunk of weight control issues. It doesn't intrinsically need a set point concept, but there is every reason to accept some brain input to determine bodyweight. But the idea that the brain can over ride the obesogenic effect of a diet which requires chronic hyperinsulinaemia to maintain a semblance of health is very hard to accept.
It was working through these concepts that I dug out a fascinating paper on leptin and blood glucose emailed to me by Stephan a little while ago. I finally got to read it in depth last week.
The streptozotocotin diabetic rat strikes me as a pretty good model for type 1 diabetes. It looks to be a pure beta cell failure model, ie it lacks the stupidity of considering metabolic freaks such as the Otsuka diabetic rat as in any way representative of any form of human type 2 diabetes. I have time for STZ diabetic rats as being a model for type 1 diabetes. STZ produces acute, persistent and profound hypoinsulinaemia.
The researchers made some rats severely diabetic with STZ (BG > 400mg/dl), then infused leptin in to the cerebrospinal fluid within the third ventricle of the brain.
End result: Normoglycaemia. No change in blood insulin level.
That's quite impressive. No, it's bloody amazing. They did a ton of other things too and had a number of excellent control groups. The conclusion the researchers reached is that there appears to be neural control of hepatic glucose synthesis and output, plus neural control of muscle glucose uptake. They're probably correct. It's a very interesting paper. But is a massive intracranial infusion of leptin genuine physiology or is it pushing a fine tuning system to its ultimate limits using a chemical gorilla? Turbocharging a Morris Minor to out-accelerate a performance BMW?
They were putting almost as much leptin per minute in to the CSF/brain volume as would be produced by whole body fat mass. They probably achieved intracerebral concentrations of leptin way above what might every be produced in plasma.
Of course the goal of the group is to produce a centrally acting leptin mimetic to treat diabetes. Hmmmm, the unintended consequences will be interesting!
As always, picking through the results tables provides a wealth of information to be fitted in to the insulinocentric view of metabolism.
Let's look at the blood insulin levels:

It looks like STZ produces profound hypoinsulinaemia. It doesn't matter what else you do, insulin is low after STZ. No problems here. Hypoinsulinaemia across the board.
Before we look at blood glucose levels let's peek at leptin levels:

Interesting? Well the rats in the control non-diabetic group have lots of leptin. Unless the rat is being given a subcutaneous infusion of leptin (right hand column) there is very little leptin in the blood stream of the diabetic rats. Why so? STZ does nothing to leptin production. But hypoinsulinaemia does a great deal to lipolysis. These rats have had uncontrolled type one diabetes for a couple of weeks before the six day experiment. We don't get any bodyweights in the paper but leptin reflects adipose tissue mass. The STZ rats are profoundly fat depleted compared to the non diabetic controls. I think they're emaciated. This thin:
"WAT [White Adipose Tissue] had clearly atrophied in size in STZ-SAL rats. WAT in STZ-LEP and STZ-PF rats was further atrophied compared with the STZ-SAL group. For that reason, we could not extract enough RNA for Northern blotting"
That's thin.
So now let's look at weight change. During the 6 day experiment the non diabetic control rats gained about 15g. The hypoinsulinaemic groups all lost 15-25g bodyweight (except the semi starved group in column 4, starvation of type one diabetics is not advised, ND for leptin in the above graph wasn't that they didn't look for leptin, it's just the amounts present where below the limits of their assay).

This is irrespective of whether they were spilling glucose through their kidneys or not. Hypoinsulinaemia allows lipolysis. Drop insulin and you drop fat, however much rat carbohydrate-crap-in-a-bag you eat. Intracerebral leptin does not stop this.
Now let's look at food intake:

STZ diabetic rats become hyperphagic. At least when they are fed on rodent chow and allowed free access. High carbohydrate, low fat. As the authors point out this does not happen if you feed a high fat diet but I've blogged about this elsewhere.
I'd just like to consider why this hyperphagia should occur from the hang-glider perspective, rather than the Eurofighter perspective.
STZ rats lack insulin. They do lipolysis to extreme levels and run their muscles on fatty acids. Until there is not a lot of fat left, as reflected by hypoleptinaemia. Down on the ground the cells needs calories but there is not enough fat left for this level of hypoinsulinaemia to provide free fatty acids for metabolism. But it is possible to get blood glucose levels high enough to use non GLUT4 transporters to get glucose into muscle cells (see here). With hyperglycaemia there is a chance of survival. To do this you need marked hyperglycaemia. You need it, so metabolism does its best to provide it. In fact these rats will have been hyperglucagonaemic to help raise their blood glucose.
So the rats will eat a ton of glucose precursor, fail to retain it in the liver due to hypoinsulinaemia, add as much to it, using glucagon, as possible and push glucose in to muscles using the brute force of a concentration gradient. The cost is calorie loss through glycosuria and whole body hyperglycaemic damage. But death is postponed. Life is tenaceous.
The STZ control rats ate over twice as much crapinabag as the non STZ controls while continuing to lose weight hand over fist.... Good old hypoinsulinaemia and the body's adaptation to it.
The paper certainly gives support to the concept that the brain is significantly involved in glucose homeostasis. How this will relate a fat mass set point is a line of thought I'm looking forward to seeing Stephan develop.
I rather like this paper. It doesn't need me to move from my insulinocentric bias for weight loss. Ah, good.
Back to LC for diabetes and adaptation to high carb next.
Peter
You sometimes have interesting conversations in reception. A lady commented to me that she had no trouble getting arthritis meds in to her dog, some difficulty with antibiotics and that there was no way that she could persuade him to take the tramadol which had been prescribed as a supplementary analgesic for his arthritis.
I mentioned that he might not find the psychotropic effects of tramadol pleasant. A bit like morphine, not everyone finds the effects enjoyable. She concurred about the effects of morphine. It turned out that she had once been given morphine after surgery and had lost her automatic ability to breathe.... A sort of iatrogenic and thankfully temporary Ondine's curse. More poetically here.
In her case the solution had been that a nurse was assigned to sit by her bed and remind her to take a breath whenever she forgot, until automaticity of breathing returned as the morphine wore off. It's a rare side effect.
It started me thinking about control systems. The pancreas monitors blood glucose and responds with insulin and glucagon. It has a generous nerve supply with a whole host of neurotransmitters affecting insulin output. There are also glucoreceptors in the aortic bodies feeding information to the autonomic nervous system. There are, not surprisingly, nuclei in the brain which have glucosensors. There are probably insulin receptors in the brain too.
I think it is just worth pointing out that I have absolutely no problem with the fact that the brain controls blood glucose. Not the pancreas, not the liver, not the adipocytes. Long term stability needs brain input. You could probably say the same about body weight.
It's an integrated system.
But I doubt very much that the brain is central to the bulk management of metabolism. You would hardly expect a regulatory system such as the pancreas/liver/glucose axis to be intrinsically unstable and only kept functional by continuous and aggressive brain intervention. Metabolism ought to be largely self regulatory, with fine tuning by the brain to meet specific conditions.
Aside: Apparently the Eurofighter is intrinsically unstable in flight and is kept stable by enormous computing power and continuous hardware activity. It uses this intrinsic instability, given tightly controlled expression, in order to flip the aircraft from zero to 7 G in a completely unreasonable period of time. Keeping the pilot conscious under these conditions is the challenge to be met. I only heard any of this because we had an interesting presentation about this latter aspect at an anaesthesia meeting on cerebral perfusion pressures not so long back... Back to metabolism:
There is clearly a regulatory set point for the control of breathing. There is also one for blood pressure, blood sodium, potassium, pretty well everything else. I manipulate many of these daily to earn a living. Why not one for bodyweight?
At the moment I have an insulinocentric view of metabolism and bodyweight. Insulin appears to explain a fairly large chunk of weight control issues. It doesn't intrinsically need a set point concept, but there is every reason to accept some brain input to determine bodyweight. But the idea that the brain can over ride the obesogenic effect of a diet which requires chronic hyperinsulinaemia to maintain a semblance of health is very hard to accept.
It was working through these concepts that I dug out a fascinating paper on leptin and blood glucose emailed to me by Stephan a little while ago. I finally got to read it in depth last week.
The streptozotocotin diabetic rat strikes me as a pretty good model for type 1 diabetes. It looks to be a pure beta cell failure model, ie it lacks the stupidity of considering metabolic freaks such as the Otsuka diabetic rat as in any way representative of any form of human type 2 diabetes. I have time for STZ diabetic rats as being a model for type 1 diabetes. STZ produces acute, persistent and profound hypoinsulinaemia.
The researchers made some rats severely diabetic with STZ (BG > 400mg/dl), then infused leptin in to the cerebrospinal fluid within the third ventricle of the brain.
End result: Normoglycaemia. No change in blood insulin level.
That's quite impressive. No, it's bloody amazing. They did a ton of other things too and had a number of excellent control groups. The conclusion the researchers reached is that there appears to be neural control of hepatic glucose synthesis and output, plus neural control of muscle glucose uptake. They're probably correct. It's a very interesting paper. But is a massive intracranial infusion of leptin genuine physiology or is it pushing a fine tuning system to its ultimate limits using a chemical gorilla? Turbocharging a Morris Minor to out-accelerate a performance BMW?
They were putting almost as much leptin per minute in to the CSF/brain volume as would be produced by whole body fat mass. They probably achieved intracerebral concentrations of leptin way above what might every be produced in plasma.
Of course the goal of the group is to produce a centrally acting leptin mimetic to treat diabetes. Hmmmm, the unintended consequences will be interesting!
As always, picking through the results tables provides a wealth of information to be fitted in to the insulinocentric view of metabolism.
Let's look at the blood insulin levels:

It looks like STZ produces profound hypoinsulinaemia. It doesn't matter what else you do, insulin is low after STZ. No problems here. Hypoinsulinaemia across the board.
Before we look at blood glucose levels let's peek at leptin levels:

Interesting? Well the rats in the control non-diabetic group have lots of leptin. Unless the rat is being given a subcutaneous infusion of leptin (right hand column) there is very little leptin in the blood stream of the diabetic rats. Why so? STZ does nothing to leptin production. But hypoinsulinaemia does a great deal to lipolysis. These rats have had uncontrolled type one diabetes for a couple of weeks before the six day experiment. We don't get any bodyweights in the paper but leptin reflects adipose tissue mass. The STZ rats are profoundly fat depleted compared to the non diabetic controls. I think they're emaciated. This thin:
"WAT [White Adipose Tissue] had clearly atrophied in size in STZ-SAL rats. WAT in STZ-LEP and STZ-PF rats was further atrophied compared with the STZ-SAL group. For that reason, we could not extract enough RNA for Northern blotting"
That's thin.
So now let's look at weight change. During the 6 day experiment the non diabetic control rats gained about 15g. The hypoinsulinaemic groups all lost 15-25g bodyweight (except the semi starved group in column 4, starvation of type one diabetics is not advised, ND for leptin in the above graph wasn't that they didn't look for leptin, it's just the amounts present where below the limits of their assay).
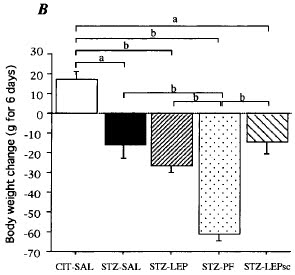
This is irrespective of whether they were spilling glucose through their kidneys or not. Hypoinsulinaemia allows lipolysis. Drop insulin and you drop fat, however much rat carbohydrate-crap-in-a-bag you eat. Intracerebral leptin does not stop this.
Now let's look at food intake:

STZ diabetic rats become hyperphagic. At least when they are fed on rodent chow and allowed free access. High carbohydrate, low fat. As the authors point out this does not happen if you feed a high fat diet but I've blogged about this elsewhere.
I'd just like to consider why this hyperphagia should occur from the hang-glider perspective, rather than the Eurofighter perspective.
STZ rats lack insulin. They do lipolysis to extreme levels and run their muscles on fatty acids. Until there is not a lot of fat left, as reflected by hypoleptinaemia. Down on the ground the cells needs calories but there is not enough fat left for this level of hypoinsulinaemia to provide free fatty acids for metabolism. But it is possible to get blood glucose levels high enough to use non GLUT4 transporters to get glucose into muscle cells (see here). With hyperglycaemia there is a chance of survival. To do this you need marked hyperglycaemia. You need it, so metabolism does its best to provide it. In fact these rats will have been hyperglucagonaemic to help raise their blood glucose.
So the rats will eat a ton of glucose precursor, fail to retain it in the liver due to hypoinsulinaemia, add as much to it, using glucagon, as possible and push glucose in to muscles using the brute force of a concentration gradient. The cost is calorie loss through glycosuria and whole body hyperglycaemic damage. But death is postponed. Life is tenaceous.
The STZ control rats ate over twice as much crapinabag as the non STZ controls while continuing to lose weight hand over fist.... Good old hypoinsulinaemia and the body's adaptation to it.
The paper certainly gives support to the concept that the brain is significantly involved in glucose homeostasis. How this will relate a fat mass set point is a line of thought I'm looking forward to seeing Stephan develop.
I rather like this paper. It doesn't need me to move from my insulinocentric bias for weight loss. Ah, good.
Back to LC for diabetes and adaptation to high carb next.
Peter
Earning a crust
We seem to have had a fair number of diabetic dogs come through work recently. Most of them have presented in ketoacidosis. This is a direct consequence of catastrophic insulin deficiency. Hypoinsulinaemia leads to unrestrained lipolysis with production of ketone bodies to the point of profound metabolic acidosis, vomiting, dehydration and risk of rapid death. Oh, and weight loss.
I keep reading snippets about the unimportance of insulin in the control of weight loss from various sources in the blogosphere, so it's sort of tempting to inhibit lipolysis with a couple of big, high calorie blocks of butter or maybe by an Intralipid infusion (yeugh, soyabean oil intravenously, disgusting). But, what the hell, I'm still a bit of a traditionalist on occasion, so I still shut down lipolysis with insulin.
It doesn't seem to matter how much insulin you inject. Once upon a time I would have reached for soluble neutral insulin and bunged it in by intramuscular injection. I had been considering changing to using a GIK (glucose/insulin/potassium) infusion for ketoacidosis but the loss of any soluble insulin preparation from the veterinary market in the UK has stopped my thoughts along those lines.
So now it's lente insulin (the only formulation we have left) by subcutaneous injection and aggressive fluid therapy to allow its absorption. Ultimately it doesn't matter. Any old insulin at almost any old dose rate will inhibit lipolysis well enough to get ketone production under control. You then start seriously supplementing with potassium while catching the hypoglycaemia with an iv glucose infusion as soon as the insulin level in the blood gets high enough to start doing things other than inhibit lipolysis..........
Replacing the missing insulin inhibits lipolysis first. As the blood insulin level increases it then shifts potassium from plasma in to cells. Still higher levels get GLUT4s on to cell surface membranes and facilitate glucose transport.
This is utterly basic A&E work.
Of course the lipolysis of weight loss might just be different from the lipolysis of ketoacidosis. I dunno. Stranger things have happened.
The other thing which has happened is that I have accumulated a couple of these patients who have turned out to be unstable diabetics. They are fascinating cases. You have to understand that as a heretic I try keep my nose out of other clinician's cases, especially diabetic dogs. The basic standard veterinary approach to diabetes is to feed your patient a meal of utter crap, mostly made of sustained release carbohydrate, and cover it with an industrial dose of 12 hour acting lente insulin. Repeat every 12 hours. You can book the cataract surgery for a year's time on the day you make the diagnosis.
The first patient, I'll call her Grace, is a spaniel with a two year history of dry eye, failure to produce tears. A sort of type one diabetes of the eye... What does dry eye have to do with diabetes? Dr Penny Watson of Cambridge Vet School gave a very perceptive presentation about chronic pancreatitis leading to diabetes at the 2010 BSAVA congress. In dogs pancreatitis is often a chronic inflammatory disease which can end up as a "type one like" diabetes syndrome or, alternatively, as an exocrine secretion deficiency giving a failure to digest food. Occasionally both. Which happens to occur in a given individual is probably a genetic lottery.
This dog had had dry eye well before her pancreatic beta cell failure. Dr Watson pointed out that dry eye is an autoimmune attack on the tear producing glands and the attack is aimed at ductal tissue. Stem cells for pancreatic beta cells are derived from pancreatic ductal tissue, which is similar enough to tear gland ductal tissue to produce an association, both diseases in the same patient. Cocker spaniels are far more commonly affected than other breeds. She had some absolutely amazing immunohistochemistry slides.
A sort of Sjögren’s Syndrome of the pancreas, probably another gift of gluten.
The other patient is a middle aged terrier, let's call him William. He has a two year history of chronic hepatopathy before presenting as a type-one-like diabetic. I'd guess he has a combination of non alcoholic fatty liver disease combined with non alcoholic fatty pancreatic disease. He was on a diet of commercial ultra crap, rice mixed with a mess of enzymically degraded protein to limit pre existing skin allergies. Imagine trying to catch the glucose spike from a bowl of white rice with a slow onset sustained release insulin. That initial spike of blood glucose was being caught, too late, with an enormous dose of lente insulin. Two hours later he would have a blood glucose of around 10mmol/l, but dropping like a stone. Suddenly the next reading would be back above 30mmol/l. Dr Bernstein doesn't have a lot of time for the Somogyi overswing. I do, certainly for this dog. The liver is loaded with glycogen, it panics and dumps a fair dose of glucose to (over) correct the incipient hypoglycaemia.
With the standard management approach both dogs had immediately come out of ketoacidosis and had gained weight over several weeks. Did I mention that insulin inhibits lipolysis? Ok, I'll drop it in to casual conversation again. Insulin inhibits lipolysis. Weight gain? Now there's a surprise. Of course there is no ketosis but also no suggestion of normoglycaemia at any stage of a 12 hour glucose curve either.
For some reason Grace had been dropped in to the middle of an afternoon consulting session for a random, post absorptive blood glucose check with me, presumably to adjust her insulin dosage. I wasn't her clinician. I think this reading was somewhere around 25mmol/l. She was ravenous, depressed and polydipsic. Next morning I had her admitted, halved her insulin and fed her a can of cat food with a carbohydrate content of approximately zero, except whatever cooked liver was in the can. The curve came down from somewhere over 35mmol/l to about 14mmol/l and stayed there. We've incremented her insulin up and are aiming for peak blood glucose below 10mmol/l and post absorptive levels below 7mmol/l. Probably the best we can do with lente insulin.
William came to me because lente plus ultracrap was giving completely random blood glucose levels. His owner had been offered referral to an endocrinologist or to see the weird in-house vet who didn't feed sugar to diabetics. That's me. They chose to see me for some reason.
He behaved similarly to Grace when fed all meat cat food and half dose insulin, which is good but we probably need better glycaemic control if we are going to get his hepatopathy to halt. We're getting post absorptive glucose levels between 5mmol/l and 7mmol/l but there is a post feeding spike to over 14mmol/l, which suggests there is a lot of liver in the cat food to provide significant glycogen in the diet. But so far he's a lot more stable now than he ever was on ultracrap.
So why low carbohydrate? Why not simply adjust insulin to cover normal diabetic crap-in-a-bag?
This comes down to the difference between exogenous insulin and pancreas secreted insulin.
Let's recap the two main functions of insulin. First is the inhibition of lipolysis, I may have mentioned this before. This bit is easy.
The next is the suppression of glucose release from the liver. This is utterly core to normoglycaemia. This is not quite so easy.
This is because insulin is normally produced by the pancreas and it travels directly to the liver. There is first pass metabolism by the liver, lots of it. The liver extracts between 50% and 80% of all of the insulin produced by the pancreas. Relatively little ever gets to the systemic circulation. This residue is what should be controlling adipocyte function.
If we turn this on its head we can say that we need to provide relatively high levels of insulin by subcutaneous injection to achieve those levels at the liver which would normally be delivered from the pancreas. But we end up not just bathing the liver with this specific high concentration of insulin. To reach "pancreatic" concentrations at the liver, from a subcutaneous injection site, we will have to hit the adipocytes far harder than we want to. We might well achieve adequate control of hepatic glucose output but at the cost of suppressed lipolysis. Weight gain. And hunger of course.
You could add in a third role for insulin as the management of dietary carbohydrate, ie portal vein glucose sequestration in to the liver and its metabolism by muscles when it spills over in to the systemic circulation. Generally I regard this as what Douglas Adams described in the Hitchiker's Guide to the Galaxy as an SEP. This is a "Somebody Else's Problem".
You want to do that? Fine, you sort out the mess.
I really have to discuss this in some detail because it is perfectly clear that non diabetic humans, so long as they have a functional physiology, can generally deal with massive amounts of carbohydrate rather well. So well that they can lose weight, rather a lot of it, by eating a diet of potatoes alone. This perfectly compatible with why LC is the logical and necessary approach to diabetes. That needs a separate post with a few links to pubmed rather than me rambling on about how I earn my living.
Peter
I keep reading snippets about the unimportance of insulin in the control of weight loss from various sources in the blogosphere, so it's sort of tempting to inhibit lipolysis with a couple of big, high calorie blocks of butter or maybe by an Intralipid infusion (yeugh, soyabean oil intravenously, disgusting). But, what the hell, I'm still a bit of a traditionalist on occasion, so I still shut down lipolysis with insulin.
It doesn't seem to matter how much insulin you inject. Once upon a time I would have reached for soluble neutral insulin and bunged it in by intramuscular injection. I had been considering changing to using a GIK (glucose/insulin/potassium) infusion for ketoacidosis but the loss of any soluble insulin preparation from the veterinary market in the UK has stopped my thoughts along those lines.
So now it's lente insulin (the only formulation we have left) by subcutaneous injection and aggressive fluid therapy to allow its absorption. Ultimately it doesn't matter. Any old insulin at almost any old dose rate will inhibit lipolysis well enough to get ketone production under control. You then start seriously supplementing with potassium while catching the hypoglycaemia with an iv glucose infusion as soon as the insulin level in the blood gets high enough to start doing things other than inhibit lipolysis..........
Replacing the missing insulin inhibits lipolysis first. As the blood insulin level increases it then shifts potassium from plasma in to cells. Still higher levels get GLUT4s on to cell surface membranes and facilitate glucose transport.
This is utterly basic A&E work.
Of course the lipolysis of weight loss might just be different from the lipolysis of ketoacidosis. I dunno. Stranger things have happened.
The other thing which has happened is that I have accumulated a couple of these patients who have turned out to be unstable diabetics. They are fascinating cases. You have to understand that as a heretic I try keep my nose out of other clinician's cases, especially diabetic dogs. The basic standard veterinary approach to diabetes is to feed your patient a meal of utter crap, mostly made of sustained release carbohydrate, and cover it with an industrial dose of 12 hour acting lente insulin. Repeat every 12 hours. You can book the cataract surgery for a year's time on the day you make the diagnosis.
The first patient, I'll call her Grace, is a spaniel with a two year history of dry eye, failure to produce tears. A sort of type one diabetes of the eye... What does dry eye have to do with diabetes? Dr Penny Watson of Cambridge Vet School gave a very perceptive presentation about chronic pancreatitis leading to diabetes at the 2010 BSAVA congress. In dogs pancreatitis is often a chronic inflammatory disease which can end up as a "type one like" diabetes syndrome or, alternatively, as an exocrine secretion deficiency giving a failure to digest food. Occasionally both. Which happens to occur in a given individual is probably a genetic lottery.
This dog had had dry eye well before her pancreatic beta cell failure. Dr Watson pointed out that dry eye is an autoimmune attack on the tear producing glands and the attack is aimed at ductal tissue. Stem cells for pancreatic beta cells are derived from pancreatic ductal tissue, which is similar enough to tear gland ductal tissue to produce an association, both diseases in the same patient. Cocker spaniels are far more commonly affected than other breeds. She had some absolutely amazing immunohistochemistry slides.
A sort of Sjögren’s Syndrome of the pancreas, probably another gift of gluten.
The other patient is a middle aged terrier, let's call him William. He has a two year history of chronic hepatopathy before presenting as a type-one-like diabetic. I'd guess he has a combination of non alcoholic fatty liver disease combined with non alcoholic fatty pancreatic disease. He was on a diet of commercial ultra crap, rice mixed with a mess of enzymically degraded protein to limit pre existing skin allergies. Imagine trying to catch the glucose spike from a bowl of white rice with a slow onset sustained release insulin. That initial spike of blood glucose was being caught, too late, with an enormous dose of lente insulin. Two hours later he would have a blood glucose of around 10mmol/l, but dropping like a stone. Suddenly the next reading would be back above 30mmol/l. Dr Bernstein doesn't have a lot of time for the Somogyi overswing. I do, certainly for this dog. The liver is loaded with glycogen, it panics and dumps a fair dose of glucose to (over) correct the incipient hypoglycaemia.
With the standard management approach both dogs had immediately come out of ketoacidosis and had gained weight over several weeks. Did I mention that insulin inhibits lipolysis? Ok, I'll drop it in to casual conversation again. Insulin inhibits lipolysis. Weight gain? Now there's a surprise. Of course there is no ketosis but also no suggestion of normoglycaemia at any stage of a 12 hour glucose curve either.
For some reason Grace had been dropped in to the middle of an afternoon consulting session for a random, post absorptive blood glucose check with me, presumably to adjust her insulin dosage. I wasn't her clinician. I think this reading was somewhere around 25mmol/l. She was ravenous, depressed and polydipsic. Next morning I had her admitted, halved her insulin and fed her a can of cat food with a carbohydrate content of approximately zero, except whatever cooked liver was in the can. The curve came down from somewhere over 35mmol/l to about 14mmol/l and stayed there. We've incremented her insulin up and are aiming for peak blood glucose below 10mmol/l and post absorptive levels below 7mmol/l. Probably the best we can do with lente insulin.
William came to me because lente plus ultracrap was giving completely random blood glucose levels. His owner had been offered referral to an endocrinologist or to see the weird in-house vet who didn't feed sugar to diabetics. That's me. They chose to see me for some reason.
He behaved similarly to Grace when fed all meat cat food and half dose insulin, which is good but we probably need better glycaemic control if we are going to get his hepatopathy to halt. We're getting post absorptive glucose levels between 5mmol/l and 7mmol/l but there is a post feeding spike to over 14mmol/l, which suggests there is a lot of liver in the cat food to provide significant glycogen in the diet. But so far he's a lot more stable now than he ever was on ultracrap.
So why low carbohydrate? Why not simply adjust insulin to cover normal diabetic crap-in-a-bag?
This comes down to the difference between exogenous insulin and pancreas secreted insulin.
Let's recap the two main functions of insulin. First is the inhibition of lipolysis, I may have mentioned this before. This bit is easy.
The next is the suppression of glucose release from the liver. This is utterly core to normoglycaemia. This is not quite so easy.
This is because insulin is normally produced by the pancreas and it travels directly to the liver. There is first pass metabolism by the liver, lots of it. The liver extracts between 50% and 80% of all of the insulin produced by the pancreas. Relatively little ever gets to the systemic circulation. This residue is what should be controlling adipocyte function.
If we turn this on its head we can say that we need to provide relatively high levels of insulin by subcutaneous injection to achieve those levels at the liver which would normally be delivered from the pancreas. But we end up not just bathing the liver with this specific high concentration of insulin. To reach "pancreatic" concentrations at the liver, from a subcutaneous injection site, we will have to hit the adipocytes far harder than we want to. We might well achieve adequate control of hepatic glucose output but at the cost of suppressed lipolysis. Weight gain. And hunger of course.
You could add in a third role for insulin as the management of dietary carbohydrate, ie portal vein glucose sequestration in to the liver and its metabolism by muscles when it spills over in to the systemic circulation. Generally I regard this as what Douglas Adams described in the Hitchiker's Guide to the Galaxy as an SEP. This is a "Somebody Else's Problem".
You want to do that? Fine, you sort out the mess.
I really have to discuss this in some detail because it is perfectly clear that non diabetic humans, so long as they have a functional physiology, can generally deal with massive amounts of carbohydrate rather well. So well that they can lose weight, rather a lot of it, by eating a diet of potatoes alone. This perfectly compatible with why LC is the logical and necessary approach to diabetes. That needs a separate post with a few links to pubmed rather than me rambling on about how I earn my living.
Peter
I have net access again, broadband rather than a mobile phone dongle with intermittent connection that would only talk to my wife's PC because my mac has not needed any sort of system update since a very long time ago!
Posts are coming and I'll try to do something with the pile of comments which need moderating with some attention and a whole stack of emails too.
Woo hoo, click and page loads, no 10 minute wait, that's good!
Posts are coming and I'll try to do something with the pile of comments which need moderating with some attention and a whole stack of emails too.
Woo hoo, click and page loads, no 10 minute wait, that's good!
Tuesday, December 28, 2010
Anacetrapib and phytotoxins
Just starting to find a little time to post. This seems like a worthwhile snippet as a follow on to the anacetrapib post, easier to put up than the cooking epics on insulin and the liver, parts two onwards........
Ok, the usual recap:
First there was cholesterol. It was bad, life was simple.
Then came Good cholesterol, HDL battling the Bad cholesterol, LDL.
Then there was Good LDL, large buoyant battling with Really Bad LDL, small dense LDL, sdLDL.
Not only that but native LDL appears to be harmless, it's only oxidised LDL which is the killer, oxLDL.
So the evil sdLDL is only really evil because it is more easily oxidised than fluffier LDL. Maybe, but in general I tend to have glazed over by now, befuddled by the blur of the moving goal posts.
But just occasionally something does grab my attention, especially if it markedly deepens the hole being dug for itself by the lipid hypothesis, like anacetrapib.
It was thanks to Dr Davis that I grasped the concept of CETP inhibitors as eliminators of sdLDL. That's what they are. If you believe in the lipid hypothesis it must be pretty interesting to have a drug which virtually eliminates sdLDL while increasing the body count for cardiovascular deaths, even if 4 dead out of 808 vs 1 dead out of 804 does not reach statistical significance.
But the real gem from Dr D was the finding that anthocyanins are CETP inhibitors. You no longer need to sign up for the next anacetrapib trial to die of a heart attack in the cause of the lipid hypothesis. You can buy a do-it-yourself CETP inhibitor in the form of a purple plant dye.
EDIT pre posting: It always amazes me that someone as perceptive on blood glucose, and indirectly on blood insulin, as Dr Davis can still believe the lipid hypothesis. Really believe. Fascinating.
There now, we all know plants are all natural, healthy and safe. Perhaps that includes recreational plants like Deadly Nightshade, Nux Vomica and Henbane. As an alternative to anacetrapib you can only hope the anthocyanins don't work!
If they do work at least you might have the consolation that you died with cracking lipids.
Peter
PS, taken from here on flavonoids, discussed here:
"However, a similar decrease in protein oxidation [on flavonoid elimination], in 8-oxo-dG excretion and in the increased resistance of plasma lipoproteins to oxidation in the present study points to a more general relief of oxidative stress after depletion of flavonoid- and ascorbate-rich fruits and vegetables from the diet, contrary to common beliefs."
Want oxidative damage? Munch those flavonoids; and the anthocyanin flavonoids come with the added toxicity of CETP inhibition. Mmmmmm, purple fruit!
Ok, the usual recap:
First there was cholesterol. It was bad, life was simple.
Then came Good cholesterol, HDL battling the Bad cholesterol, LDL.
Then there was Good LDL, large buoyant battling with Really Bad LDL, small dense LDL, sdLDL.
Not only that but native LDL appears to be harmless, it's only oxidised LDL which is the killer, oxLDL.
So the evil sdLDL is only really evil because it is more easily oxidised than fluffier LDL. Maybe, but in general I tend to have glazed over by now, befuddled by the blur of the moving goal posts.
But just occasionally something does grab my attention, especially if it markedly deepens the hole being dug for itself by the lipid hypothesis, like anacetrapib.
It was thanks to Dr Davis that I grasped the concept of CETP inhibitors as eliminators of sdLDL. That's what they are. If you believe in the lipid hypothesis it must be pretty interesting to have a drug which virtually eliminates sdLDL while increasing the body count for cardiovascular deaths, even if 4 dead out of 808 vs 1 dead out of 804 does not reach statistical significance.
But the real gem from Dr D was the finding that anthocyanins are CETP inhibitors. You no longer need to sign up for the next anacetrapib trial to die of a heart attack in the cause of the lipid hypothesis. You can buy a do-it-yourself CETP inhibitor in the form of a purple plant dye.
EDIT pre posting: It always amazes me that someone as perceptive on blood glucose, and indirectly on blood insulin, as Dr Davis can still believe the lipid hypothesis. Really believe. Fascinating.
There now, we all know plants are all natural, healthy and safe. Perhaps that includes recreational plants like Deadly Nightshade, Nux Vomica and Henbane. As an alternative to anacetrapib you can only hope the anthocyanins don't work!
If they do work at least you might have the consolation that you died with cracking lipids.
Peter
PS, taken from here on flavonoids, discussed here:
"However, a similar decrease in protein oxidation [on flavonoid elimination], in 8-oxo-dG excretion and in the increased resistance of plasma lipoproteins to oxidation in the present study points to a more general relief of oxidative stress after depletion of flavonoid- and ascorbate-rich fruits and vegetables from the diet, contrary to common beliefs."
Want oxidative damage? Munch those flavonoids; and the anthocyanin flavonoids come with the added toxicity of CETP inhibition. Mmmmmm, purple fruit!
Subscribe to:
Posts (Atom)
