Tucker has a podcast episode in which he chats to John Speakman about obesity. It's one of the more interesting podcasts I've listened to in many years.
Ep. 22: John Speakman—What Causes Obesity?
A very large part of the core discussion is contained within this paper, a massive collaboration, with Speakman as first author:
Total daily energy expenditure has declined over the last 3 decades due to declining basal expenditure not reduced activity expenditureEp. 22: John Speakman—What Causes Obesity?
A very large part of the core discussion is contained within this paper, a massive collaboration, with Speakman as first author:
Basically total daily energy expenditure in the studied populations is down slightly over the last 30 years, despite daily activity energy expenditure going up. This means that basal metabolic rate must have dropped.
Which, of course, begs the question of what might cause basal metabolic rate to fall.
The answer is not obesity.
There are certain groups of people who *do* have a decreased BMR, the most obvious of whom are the post-obese.
The post-obese, like the pre-obese, come with a cluster of abnormalities the two most prominent of which are an enhanced insulin sensitivity and a defect in fat oxidation. And sometimes a depressed metabolic rate, especially BMR.
To me, the enhance insulin sensitivity is causal, the impaired fat oxidation is secondary. The decreased metabolic rate is simply a longer term downstream effect of chronic under supply of calories to metabolism.
Aside: I haven't discussed it yet but, obviously, pathological insulin sensitivity should also show as an exaggerated ability to over-store fat under peak insulin effect. This shows rather nicely under an hyperinsulinaemic euglycaemic clamp in Astup's lab. See top panel of Fig 2. But currently I'm mostly thinking about fasting conditions. End aside.
So. The core feature of pre or post obesity following on from the pathological insulin sensitivity is a decreased ability to oxidise lipid and a facilitated ability to oxidise carbohydrate. The RQ should rise.
What would happen if you took eight apparently healthy men and fed them, for a week, a complete diet providing 2% PUFA then switched them to a 10% PUFA diet for another week, as a crossover study?
This is the paper, from 1988:
Polyunsaturated:Saturated Ratio of Diet Fat Influences Energy Substrate Utilization in the Human
You can clearly alter the RQ under fasting conditions, on a fixed food quotient diet, simply by altering the dietary fat from 2% of calories as PUFA to 10% PUFA, switching palmitate in or out to balance the PUFA, which was mostly linoleic acid. MUFA were kept constant, as were all other macros.
Polyunsaturated:Saturated Ratio of Diet Fat Influences Energy Substrate Utilization in the Human
You can clearly alter the RQ under fasting conditions, on a fixed food quotient diet, simply by altering the dietary fat from 2% of calories as PUFA to 10% PUFA, switching palmitate in or out to balance the PUFA, which was mostly linoleic acid. MUFA were kept constant, as were all other macros.
Within seven days this happened to the fasting RQ values.
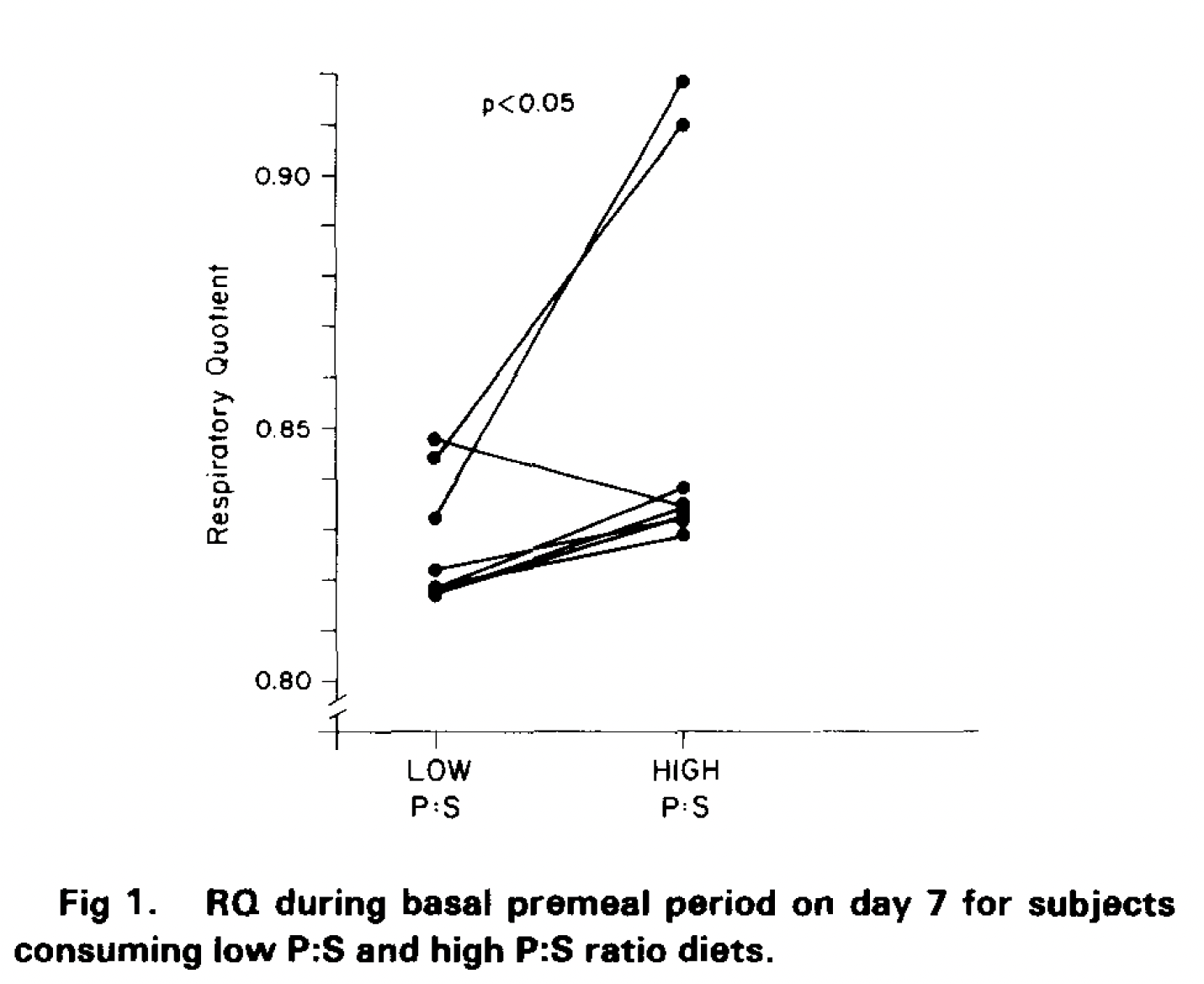
Obviously there are three interesting subjects. One showed a decrease in RQ, suggesting enhanced lipid oxidation under linoleic acid. That's unusual. It is normal for linoleic acid to augment the thermic effect of food because it is preferentially oxidised but that is finished well before an overnight fast is finished. Hard to say what was going on with that subject. It wasn't a hospitalised study but all food was provided by the investigators. File it under odd.
The rise in RQ, signifying a change away from lipid and towards carbohydrate oxidation while fasting, was (pax the exception) ubiquitous across all other subjects, but in two subjects there was such a rise in RQ that the investigators seriously considered that there might be a problem with their measurement system. There wasn't. Their comment:
"Although a fasting RQ of 0.9 is unusual, reanalysis of the calibration parameters of the respiratory gas exchange system obtained prior to tests on these subjects revealed no abnormality in analyzer response. No reason for rejection of these RQ values could be determined."
Clearly 10% of LA in the diet moves almost all subjects towards a "pre-obese" phenotype. In two of the eight this move was dramatic. It seems very, very likely to me that these two individuals are at serious risk of obesity in an omega-6 rich environment. Follow up weights over the years would have been lovely but was not remotely the purpose of the study.
Clearly 10% of LA in the diet moves almost all subjects towards a "pre-obese" phenotype. In two of the eight this move was dramatic. It seems very, very likely to me that these two individuals are at serious risk of obesity in an omega-6 rich environment. Follow up weights over the years would have been lovely but was not remotely the purpose of the study.
You can, within seven days, convert normal people in to pre-obese people, as viewed from metabolic substrate oxidation perspective.
All you have to do is make sure they are eating 10% of their calories from linoleic acid.
Some people will get bitten by this feature of linoleic acid more rapidly than others.
Eventually the whole population will.
Thank your cardiologist.
Peter
Addendum. The world is full of U shaped curves. Adding linoleic acid to the diet causes an initial excess insulin sensitivity. This distends adipocytes. As adipocytes distend they increase their basal lipolysis and release FFAs which cannot be suppressed by insulin. This, at some point, appears to normalise fasting insulin sensitivity at the cost of distended adipocytes, ie obesity, and chronically elevated FFAs. On a starch based diet the high level of post prandial insulin needed to overcome the still (unsupressable) FFA induced insulin resistance at peak absortption will sequester more lipid in to adipocytes, from where they will again leak, via basal lipolysis, leading to frank insulin resistance, hyperinsulinaemia and metabolic syndrome.
Under fasting conditions the pathological insulin sensitivity activates malonyl-CoA formation and the subsequent inhibition of CPT1 mediated entry of fatty acids in to mitochondria. This would, if it occurred in isolation, simply lead to hypometabolism unless enough glucose alone was available to run metabolism. However, it doesn't happen in isolation. It happens combined with obesity, which increases the supply of FFAs irrespective of insulin sensitivity. All that is needed is to elevate FFAs high enough to get adequate substrate in to mitochondria (there is not 100% inhibition of CPT1) and enough lipid derived ROS can then inhibit insulin, reactivate CPT1 and restore metabolism. Hence obese people have high metabolic rates.
The crux comes with conventional dieting. As adipocytes shrink the supply of FFAs from basal lipolysis drops, insulin sensitivity is restored and people get right back to where linoleic acid takes them: obtunded fat oxidation, carbohydrate dependency and hypometabolism. The classical post-diet hungry person.
Why is BMR falling in the developed world despite obesity being rampant? Because everyone is being drugged with linoleic acid to become obese and no one wants to be fat. The more you resist obesity, the more your caloric restriction shows as decreased BMR. The BMR is falling in response to Weight Watchers, Slimming World etc. People are not as fat as linoleic acid "wants" them to be.
Ultimately obesity "fixes" the pathological insulin sensitivity from linoleic acid on both fronts, at the cost of weight gain. But it's not a real fix, it's a sticking plaster and we call it metabolic syndrome.
End.

17 comments:
Dammit, I had that paper in my DB as a note "Download these..." From Astrup's 2003 paper. So little time!
Reading Jones now...
Astrup's post-obese people are a heterogenous set of groups. Each study has it's own post-obese group and they vary from really post obese to fairly post obese. And, of course, over 30 years the background LA content has risen and so might the LA content of the hospital meal the night before BMR measurement... I have a set of four papers with four post obese groups which might make an interesting blog post, one day maybe...
Peter, do you have explanation, what mechanism could make the pathological insulin sensitivity? It looks like position of unsaturated bond makes the difference. So I think it's 2,4-dienoyl-CoA reductase, DECR is involved.
Jaromir
https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.05-3953fje
Just ROS. ie a reduced input of FAD2H at mtETFdh gives too little RET to disable insulin signalling when fat oxidation w/o insulin signalling should be happening. The actual overlays seem less important to me than the underlying core signalling process. 4 billion years is a lot of time to refine the system but the basics are always preserved.
Hmm, I think the position change preserves the same FADH2/NADH ratio, but dramatically influence NADPH/NADP+ flow. See the paper, elevated gluconeogenesis, elevated cytosolic IDH1 (NADP+ dependant), suppressed IDH3, probably reversed IDH2 (NADPH dependant in reverse). DECR is NADPH dependant. How you explain it with ROS only?
Interesting paper. A couple of points, I've not come across papers where rumenic acid, cis9 trans 11 causes weight loss but if it did it I would assume it induced uncoupling, ie no elevated FFAs/trigs/liver fat etc. Cis10 trans12 is a classical lipolytic and I would routine expect it to use ROS to force lipolysis irrespective of insulin levels, hence the damage markers found.
Most papers have rumenic acid as neutral re weight and the industrial cis10 trans 12 to be weight reducing, so the paper is slightly odd. The mechanism for ROS generation by the latter is not something I've checked out as it is a modern synthetic drug not generally found outside of an industrial partial hydrogenation reactor...
I would also see rumenic acid as neutral and better control, linoleic as slightly bad and cis10 trans12 as more bad, sorted by even double bonds count. Even double bonds makes NADPH disregulation, that's the simplest explanation, but I surely could be wrong.
@mct4health: One of the complications of these unsaturated fats is that the mitochondria do not process them, they are pre-processed in the peroxisomes:
“The 24DCR [DECR1] is involved in the metabolism of all unsaturated fatty acids with double bonds originating at even-numbered positions (15, 16) and the majority of unsaturated fatty acids with double bonds originating at odd-numbered positions (17, 18), regardless of the stereochemical configuration of the double bonds.”
Fillgrove, K. L., & Anderson, V. E. (2001). The Mechanism of Dienoyl-CoA Reduction by 2,4-Dienoyl-CoA Reductase Is Stepwise: Observation of a Dienolate Intermediate. Biochemistry, 40(41), 12412–12421. https://doi.org/10.1021/bi0111606
Human peroxisomal disorders are characterized by high levels of LA, as the mitochondria won't oxidize it.
Unfortunately, I don't understand Peter's Protons model well enough to understand how this impacts it, or most of what that paper is talking about. :<
@Tucker: Linoleic acid is wery well processed by PPARa KO mice, so in mitochondria, and this is the problem. Peroxisomal metabolism is protective, it slow down glucose processing via lack of cytosolic NAD+ and fats are processed partially to acetate in peroxisomes, also protective. LA can be processed mainly in mitochondria and NADP+ can feed NNT to be converted to NAD+ and via malate aspartate shuttle support glycolysis, this I see as the pathological insulin sensitivity. NADP+ can feed IDH2 and overload TCA cycle. It might work even without insulin only via ROS. After insulin stimulation hypoglycemia occures in mice with very slow recovery. Protective fat synthesis has to be switched on, with known consequences. That's why combination of LA with ALA is less poisonous, it activates protective peroxisomal metabolism. Also MCT oil activates omega oxidation and dicarboxylic acids activates peroxisomal metabolism.
https://doi.org/10.1016/j.jnutbio.2021.108751
"Linoleic acid is wery well processed by PPARa KO mice, so in mitochondria, and this is the problem."
Do you have a link? I know for sure it doesn't happen that way in humans, which is what we really care about.
And it doesn't seem to happen in mice...
"Mitochondrial 2,4-dienoyl-CoA Reductase Deficiency in Mice Results in Severe Hypoglycemia with Stress Intolerance and Unimpaired Ketogenesis"
10.1371/journal.pgen.1000543
Tucker, are you sure LA cannot be processed in mitochondria? The link I put above is with PPARa KO mice. I comment it with pictures from it here
https://mct4health.blogspot.com/2023/11/is-coconut-oil-safe-what-about-soy-or.html
There may be some backup plan, but...
"“All peroxisomal disorders had increased brain levels of the w6 precursor, linoleic acid (18: 2w6).”
Martinez, M. (1992). Abnormal Profiles of Polyunsaturated Fatty Acids in the Brain, Liver, Kidney and Retina of Patients with Peroxisomal Disorders. Brain Research, 583(1), 171–182. https://doi.org/10.1016/S0006-8993(10)80021-6
Thank you for doi, isn't it interesting that C22:4n-6 isn't elevated at all? C22:5n-6 level is even lower! In human LCAD is missing and VLCAD is active, so may be elongated LA can be processed better in human mitochondria. Mice don't have to wait for elongation, they have plenty of LCAD.
doi:10.1016/j.bbalip.2009.05.006.
A miracle! Nature journal notes success of Keto diet in beating down pancreatic cancer (unfortunately in mice).
The growth of pancreatic tumours was diminished when mice were fed a ketogenic diet and given the P-eIF4E inhibitor tomivosertib. By depriving the body of carbohydrates, the ketogenic diet made fat-derived ketones the main energy source available to cancer cells. But the drug prevented cancer cells from extracting energy from ketones by blocking the P-eIF4E protein involved in ketone metabolism. “This unveiled a new point of vulnerability for pancreatic cancer… providing the rationale for a new combinatorial diet and small-molecule cancer
https://www.nature.com/articles/s41586-024-07781-7.epdf?sharing_token=FZ1Naq7H5uYTpW9U15zcjdRgN0jAjWel9jnR3ZoTv0MhtAxABjWjzWCNh0lR8bl7Jg48ByXOvhuJ6hUtksttZgpqKxySMNZmdtYozQA6eGKdf8otT5T7tFVqd3c0PJEcJ97AOv7MHpyxQFBNLJ5ZwwqWBFZbm5-3DVfsi2_Uv-o%3D
Gyan, £14.99 to find out if it was F3666 they used! If so it can be markedly improved on by getting rid of the linoleic acid.
Dispiriting that the cancer can utilize ketones and thus additional drug required to block the ketone-uptake pathway.
Cancer is the response to an unremitting signal to grow. I consider the signal is probably ROS derived plus subsequent metabolites (4-HNE, 13-HODE etc). Given an unremitting signal to grow a cancer cell will adopt any metabolic loophole to obey.
Post a Comment