I feel Amber articulated the adipo-centric view rather well. The whole podcast reminded me of a few ideas I've had kicking around for ages and it might now be time to do a bit more posting.
I was taken back to good old Rimonabant by some of Tucker's points. It got a passing mention in an old blog post back in 2010. I may not have been terribly impressed at the time.
Rimonabant and hemopressin
For those of us with an adipocentric/insulin based outlook on life Rimonabant is interesting. It takes about 30 seconds on PubMed to pull out
Rimonabant and hemopressin
For those of us with an adipocentric/insulin based outlook on life Rimonabant is interesting. It takes about 30 seconds on PubMed to pull out
CB1 agonists make adipocytes insulin sensitive. Rimonabant blocks this effect, which made me feel good about Protons/insulin/obesity and I left the subject alone in a nice glow of confirmation bias for a few months.
But these are isolated cells, does anything like this happen in real life? I would expect Rimonabant -> adipocytes -> reduced insulin signalling -> release of free fatty acids -> weight loss -> reduced appetite.
In that order.
Central to this is that the brain senses energy availability (Amber cited work I'd never heard of, my own ideas are just ideas. I felt it was self evident. You could say I just made it up) and reduces appetite when energy availability is good. Rimonabant frees up calories from adipocytes. But it is nasty stuff in the brain.
Developing drugs which do not pass the blood brain barrier is old hat in anaesthesia. Doing the same for CB1 receptor blockers seems pretty simple too. Just imagine, all the weight loss, none of the suicidal ideation. There are several under development.
But peripheral CB1 blocking drugs hit all sorts of targets ranging from the gut through the liver to the vagus nerve. And adipocytes.
What would an adipo-centrist look for?
Obviously we want an adipocyte specific CB1 receptor knockout mouse. It just has to dawn on you that that is what you want. Which took a while in my case.
So another 30 seconds on PubMed gave me this one:
Adipocyte cannabinoid CB1 receptor deficiency alleviates high fat diet induced memory deficit, depressive-like behavior, neuroinflammation and impairment in adult neurogenesis
and a little wander to the Place-which-shall-not-be-named gets you the full text.
Adipocyte cannabinoid CB1 receptor deficiency alleviates high fat diet induced memory deficit, depressive-like behavior, neuroinflammation and impairment in adult neurogenesis
and a little wander to the Place-which-shall-not-be-named gets you the full text.
They built a mouse model with a tamoxifen trigger-able deletion of the CB1 gene, specifically in adipocytes. How the hell they do that I can't follow but it's in the methods with links (not followed by me this time I'm afraid). I just have to accept that they can do it and that the technique is very, very clever. Then they fed a German high fat, high linoleic acid diet (around 10% calories from LA, ballpark) to make the mice fat over several months, leading to the start point at week 17 of graph E below. Then they injected tamoxifen daily for 10 days to induce permanent deletion of the CB1 receptor gene in adipocytes only. Here's what happened to the weights.
Black squares are fat mice which keep their CB1 receptors. Open squares are fat mice which lose them. D Both diamonds are controls:
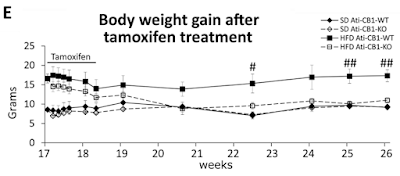
Nothing changes in the gut. Nothing changes in the liver. Nothing changes in the brain. The hypothalamic Reward™ dopaminergic neurons are left untouched. All that happens is that adipocytes lose (at least) the insulin sensitising effect of CB1 receptor activation. Weight completely normalises in less than a month. It's also worth noting that in control mice adipocyte CB1 gene deletion does nothing.
Ultimately the adipo-centric view has phenomenal explanatory power when backed up by the insulin ROS concept. Everything else is higher level signalling and unexciting to me.
There are other interesting things in the paper relating to food intake and uncoupling (ie the rapid weight normalisation occurred without reduction in food intake) but I'll call it a day for now. Except to mention that in human victims of Rimonabant it is well recognised weight loss is greater than can be accounted for by reduction in food intake. Fascinating.
At some time I'll drag myself back to working out the F:N ratio of mixed fats. Two different butters, two lards, one plus 5% soybean oil, done so far. Still got coconut oil and fully hydrogenated coconut oil to go. Losing the will to live.
Perhaps I should ask my son to write me a bit of software to do this!
Peter
