which has this excellent table showing some degree of vaccine efficacy:
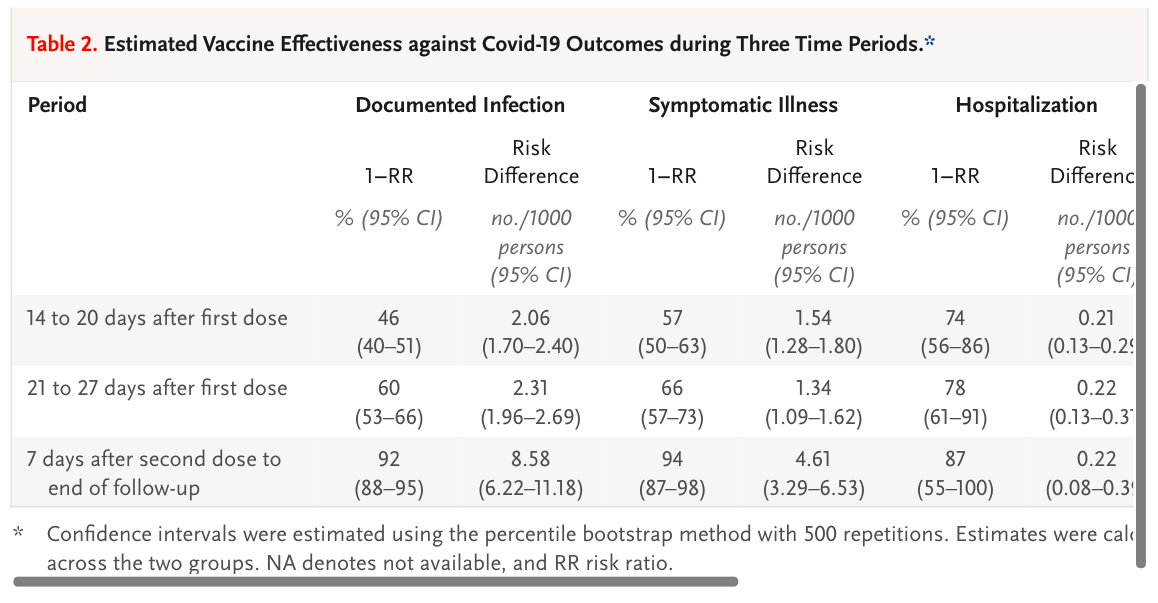
Which, understandably, only starts at 14 days after first vaccination. No one would expect a vaccine to generate immunity sooner than 14 days. So we don't need to look at those initial 14 days. Interestingly, as well as excluding the first 14 days, they also excluded 26,000 care-home/housebound people and 25,000 health care workers, I've no idea why. I'd be really interested to see how the vaccine worked in elderly "crumbly" people and those who cared for them. But that's just me.
This next snippet is just a pre-print, and might stay that way. They simply reverse engineered one of the graphs in the above paper, did some basic calculations on the numbers at-risk vs infected and extracted the incidence of PCR positivity, "cases", in the earliest days of the vaccine roll out
and found, surprisingly, that people were more likely to test positive for SARS-CoV-2 in the two weeks after the vaccine compared to the non-vaccinated arm. The risk doubles. Like this:

There is a slightly sideways suggestion as to why this might occur:
"But there was a strong increase in incidence over the first week after the injection. If the increase in incidence during the first few days after immunization is a result of people being less careful after they have had their first injection, then the vaccine effectiveness after a single dose may be even greater."
ie people might have been rather less careful than they should been for the first week after the vaccine. Those Israelis are such party animals.
"But there was a strong increase in incidence over the first week after the injection. If the increase in incidence during the first few days after immunization is a result of people being less careful after they have had their first injection, then the vaccine effectiveness after a single dose may be even greater."
ie people might have been rather less careful than they should been for the first week after the vaccine. Those Israelis are such party animals.
Now I've just picked up this peer reviewed study via twitter, again extracted from Israeli mass vaccination data:
Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine
Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine
looking at the viral load as assessed by PCR cycle threshold, from day 1 onwards after vaccination:

These people are looking at the PCR cycle threshold value for a positive test as a surrogate for viral load, ie how badly infected a person might be. Obviously, the lower the CT value the more virus is present. It just struck me that people presenting with a requirement for PCR testing 3 days after their vaccine had twice the viral load (CT drops from 25 to 24, ie a doubling of viral load) than at any other time point. This might be random chance, but may not be.
Next we can look at the elderly people in care homes in Denmark (again just a pre-print, but less controversial this time):

Incidence went up from 488 before vaccination to 760 in the first two weeks after vaccination, before improving progressively there-after. You can see in the right hand columns for vaccine efficacy that the two weeks after vaccination show a negative efficacy value.
Not to be left out, the UK did the same as Israel and Denmark:
Impact of vaccination on SARS-CoV-2 cases in the community: a population-based study using the UK’s COVID-19 Infection Survey
Impact of vaccination on SARS-CoV-2 cases in the community: a population-based study using the UK’s COVID-19 Infection Survey
but this time included the AZ vector vaccine too, this will be a generic effect.
Not so easy to make out in this study, everything is expressed in Odds Ratios, ie your risk of getting infected. Non-vaccinated individuals are considered at baseline risk, ie an OR 1.0 and are highlighted with a red circle. Just being "about to be vaccinated" people (blue circle) is massively protective. I know that sounds bizarre but the baseline and pre-vaccine people will be at differing times and infection rates vary greatly over time. A falling rate of population infection (due to Gompertz/seasonality, which control everything) is massively protective against infection. Being alive after the January peak is highly protective compared to living through the December rise.

Anyhoo, we next have days 0-7 post vaccine (green arrow), higher OR of testing positive soon after your vaccine. This worsens to the blue arrowed value for days 8-20 post vaccine before the vaccine finally kicks in as shown by the yellow arrow. I'm not going to criticise the vaccine but the yellow "arrow of success" looks pretty close to the blue circle of "about to be vaccinated". Fascinating.
This is one of the first assessments of the Pfizer vaccine from way back:
Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates

The Pfizer vaccine is marketed at the 30microgram dose rate, that's the brown plots. Over days 1-3 the lymphocyte count drops precipitously. If I have a patient on chemo whose lymphocytes have dropped below 1.0 10^9/l I would be worrying about immunosuppression. The effect is gone by a week. They never checked if it happens after the second dose.
and this is supplementary figure S3 section a

The Pfizer vaccine is marketed at the 30microgram dose rate, that's the brown plots. Over days 1-3 the lymphocyte count drops precipitously. If I have a patient on chemo whose lymphocytes have dropped below 1.0 10^9/l I would be worrying about immunosuppression. The effect is gone by a week. They never checked if it happens after the second dose.
Edit:
It has been pointed out to me that figure S3a is actually BNT162b1 and the vaccine actually selected for marketing was (sensibly) BNT162b2, which has a much milder effect on the lymphocyte count. So I have to consider that lymphopaenia might not be the mechanism or, if it is still the mechanism, it will only apply to those at the lower end of the box and whisker plots. The plots from BNT162b2 are here, first in 18-55 year olds:

It has been pointed out to me that figure S3a is actually BNT162b1 and the vaccine actually selected for marketing was (sensibly) BNT162b2, which has a much milder effect on the lymphocyte count. So I have to consider that lymphopaenia might not be the mechanism or, if it is still the mechanism, it will only apply to those at the lower end of the box and whisker plots. The plots from BNT162b2 are here, first in 18-55 year olds:

and here for the over 55 year olds

showing a very minor effect. I still ponder whether this might have a significant effect but obviously that question is wide open. The increased infection rate is too generic to be fluke, the question is more how relevant lymphopaenia might be as an explanation.
End edit.

showing a very minor effect. I still ponder whether this might have a significant effect but obviously that question is wide open. The increased infection rate is too generic to be fluke, the question is more how relevant lymphopaenia might be as an explanation.
End edit.
Lymphocytes come in many flavours. Some are irrelevant to dealing with acute infections, some are critical. On initial exposure to a virus it is the non-specific parts of the immune system which save your life in the first few days. Never mind B cells or T cells, they are critical for long term effects. In the acute phase, where the immune system has met an unknown pathogen, it's lymphocytes like natural killer cells that are going to save you. It is impossible to overstate the critical nature of the lymphocytes of the innate arm of the immune system.
To differentiate T cells from B cells from NK cells requires immunohistochemistry. This wasn't done because the lymphopaenia was considered to be transient and of no clinical significance. Bloody hell.
Lymphocytes aren't there at normal levels in the first few days after a mRNA vaccination.
To get ill you still need to meet the virus. You will still look just like a COVID-19 case, who was "probably incubating" at the time of vaccination, or went out partying under lockdown on the day you got your shot. You will still come up positive on PCR, probably with a high viral load showing as a positive result at a low cycle threshold. You might still die.
All because you were acutely immunosuppressed when you met the virus. By the vaccine. Only for a few days.
Just a little browse through Pubmed-land pulls up fresh herpes infection in people already on immunosuppressive drugs for arthritis (Israel again) after COVID-19 vaccination. Some nasty pictures in the paper
Herpes zoster following BNT162b2 mRNA Covid-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: a case series
Herpes zoster following BNT162b2 mRNA Covid-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: a case series
and also, browsing the FDA commentary on the early trials
Emergency Use Authorization (EUA) for an Unapproved Product Review Memorandum
I picked up this line:
"Suspected COVID-19 cases that occurred within 7 days after any vaccination were 409 in the vaccine group vs. 287 in the placebo group."
"Suspected COVID-19 cases that occurred within 7 days after any vaccination were 409 in the vaccine group vs. 287 in the placebo group."
These are people who looked like they had COVID-19 soon after vaccination but did not. They were PCR tested (sometimes very repeatedly) at high PCRct and were always negative. Call them ILI, influenza like illnesses. An excess in the week after vaccination occurred. Supportive of an acute immunosuppression post vaccination. It's usually SARS-CoV-2 that gets you but any other bug can do the job too.
Does any of this matter?
Maybe.
Here in the UK we had a wave of COVID-19 sweep much of the country in the spring 0f 2020. It ended largely due to the end of the winter respiratory virus season and it failed to fully penetrate to the north of England. The virus went on vacation in the summer, as respiratory viruses do. There was a finishing off of the first wave in the autumn, mostly in the northwest then the northeast. Then it started to peter out through November.
Personally I was expecting a mild winter respiratory virus season because the gross mis-management of the situation in nursing homes earlier in the year meant that many of the people who would normally have been going to die of influenza over Christmas had already been killed in the first COVID wave and its autumn residuals. And there was minimal influenza.
This didn't happen. In early December there was a modest upswing in cases, of COVID-19 this year as it was the dominant virus at the time. Then in mid December all hell broke loose.
It didn't matter what the COVID incidence was doing at a given location; it could be stable, rising or falling, there was a surge. It was big and the shape of the surge was exactly the same in all areas. The data came and went on twitter and I never screen-shotted it. Someone recently put up a related graph of the percentage positive tests which is okay but doesn't show the spectacular shape and synchrony of the absolute numbers of positive PCR test results. Here's the picture I have, best I can find:

And here the red line marks the start of vaccination roll-out and the blue line marks the start of the surge:

Here's the graph stretched out a little to show the linear rise in positivity, in all areas, over less than a week:

I'd forgotten about these weird sudden implausible rises in infection. I'd assumed the government had changed something about the PCR protocol (which they did do in December, to catch the B117 variant which spectacularly failed to kill everyone in Kent). What rekindled my interest was India.
I think these graphs are from Ted Petrou on twitter

The rises are not as synchronous as they were in the UK last December but the shape of the curves at the right hand end of the graphs is remarkably familiar. India is huge. Vaccine roll out will not be as synchronous as it was on our tiny island off the coast of Europe. Whatever India was doing before their vaccine roll out, maybe they should have just stuck with that.
A bit of an addendum:
In the UK we largely know when people received their vaccine doses, after all they're going to be needed for vaccination passports for as long as Bojo feels like imposing them. Probably for ever.
I never, ever, expected to see what vaccination does to illness, hospitalisation and death over the first few weeks because I was pretty sure it would be appalling. It was.
So I'm utterly amazed to see this:
The study is looking at hospitalisations and deaths related to time since vaccination in a cohort being followed as part of the study. You have to be ill enough to be hospitalised to be in the study so this helpfully excludes those massive numbers of false positive PCR results being generated in December before the PCRct was finally dropped from over 40 to a more reasonable 30 (still too high). These people were ill, and they were ill with SARS-CoV-2. Genuine cases as opposed to "cases".

"Given that the median incubation period is 5 days, the distribution indicates that most vaccinated hospitalised patients were infected around the time of vaccination, and the remainder after vaccination but before immunity had developed"
Also included is what happened to anyone's granny (A UK tier 2 category patient) if she picked up SARS-CoV-2 in the immediate aftermath of her vaccine. About 10% of these tier 2 patients didn't survive.

How could vaccination trigger infection? CO-CIN state the normal explanation:
"Elderly and vulnerable people who had been shielding, may have inadvertently been exposed and infected either through the end-to-end process of vaccination, or shortly after vaccination through behavioural changes where they wrongly assume they are immune"
Which translates as they got infected at their vaccination centre. Or these elderly people went to Israeli-style parties, during lockdown, starting on the day of their first vaccine dose. Wild things, those folks in nursing homes.
We had a winter resurgence of COVID-19. It became an epic disaster as a direct result of the immunosuppressive vaccine program being started while SARS-CoV-2 was the prevalent virus. People went through a vaccine centre where SARS-CoV-2 was persisting in aerosol form in the local environment.
No one seems to have considered that the vaccine might be directly immunosuppressive. For young fit healthy people this might not matter. In a nursing home it's a death sentence for many. They died.
Someone needs to tell the Indian government. And maybe the Japanese government too, before they cancel the Olympics.
I hope we're all enjoying being part of a global drug trial based on 40,000 fit healthy people observed for two months in mid summer. The UK government is, as in Israel, going to coerce any unwilling "volunteers" to make them take part in this on-going experiment. Thank goodness we have the Nuremberg Code, for what that is worth here.
Peter
PS, from Australia:
"Western Australia's latest cases stem from a hotel quarantine security guard in his 20s who has tested positive to COVID-19 and was potentially infectious in the community for four days.
State health authorities said the guard, who recently received his first dose of the Pfizer COVID-19 vaccine, worked on the same floor as two other positive cases from the United States and Indonesia."
State health authorities said the guard, who recently received his first dose of the Pfizer COVID-19 vaccine, worked on the same floor as two other positive cases from the United States and Indonesia."
No laughing. It's not funny.

111 comments:
Remember Peter, the benefits outweigh the risks, lmfao.
That is, the benefits to their tax revenues outweigh the risks of some young healthy people's heads exploding.
It's the tragedy of the commons in reverse :)
@Peter, Love it, love it, love it. I just wish I could pump my utter frustration into the clear and concise logic that you are able to muster. Thank you.
All my instincts have been to avoid the vaccine (as a healthy 56 yr old). But I was starting to waver (colleagues at work in Zoom calls talking about it endlessly, more and more family members succumbing to vaccine pressure). Thank you for the post Peter. Will stick to my guns.
Any speculation about how the vaccines suppress the immune system? I know things like Lyme bacyerium borrelia suppresses your immune system during an early acute infection, but since many of the Covid vaccines are mRNA and only code for the spike proteins, presumably in this case the effect has something to do with the immune system itself? Of course, what do I know…
cave, we don't know but I'm assuming it's consumptive. If there is a sudden massive show of viral spike protein the innate immune system will go in to overdrive. My guess would be that the general supply of NK cells gets used up and takes several days to replenish. This happens with platelets and internal bleeding. Last haemangiosarcoma we took out of a dog had used up it's platelets trying to stop the spleen bleeding. Count was 22 of whatever units platelets are measured in. Usual count 200-400... It did fine but the histopathology report is gloomy in the extreme. So there are precedents. I doubt the second vacc does the same because B and T cells will do the heavy lifting by then and they will already be in overdrive.
That's also why I think it will be generic to all mRNA vaccines. Probably safe in mid summer.
It's also fascinating that at least one member of the UK JCVI (Joint Committee on Vaccination and Immunisation) describes the committee members as struggling with conscience. In the Financial Times. They know all of the above. They know kids are going to die from the vaccine too.
Us lockdown sceptics are desperate for the vaccine to work. No one wants rule by fiat from Bojo for eternity (other than Bojo and cronies of course!).
Peter
The production of billions of spike proteins and then antibodies is naturally a drain on energy supplies and the mitochondria are going to take a hit!
https://www.salk.edu/news-release/the-novel-coronavirus-spike-protein-plays-additional-key-role-in-illness/?s=09
I strongly suspect the vaccine depletes Vit D levels and weakens the immune system.
Lots of potions!
Peter
I mean options!
Peter
Maybe the peak of the covid wave wasn't the best time to vaccinate seniors.
Vitamin D status could play a role? Covid and the Covid-vaccine eats your vit D? If you have a good status, less problems?
See for instance:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738984/
https://pubmed.ncbi.nlm.nih.gov/23556539/#:~:text=The%20mechanism%20by%20which%20high,thrombocytopenia%20or%20other%20autoimmune%20diseases
https://library.ehaweb.org/eha/2018/stockholm/216814/christopher.tham.immune.thrombocytopenia.and.vitamin.d.deficiency.html?f=media=1
Confounders ahead... Lymphocytopenia is common on infection with anything, likely a failure of the imagination to realize they are onsite doing their jobs as opposed to being in general circulation? I think I would chalk this up to the (un)healthy user bias seen in most epi studies, folks still have to alter their behavior to get exposed to get infected.
I wondered what else was in the injection:
https://portal.ct.gov/-/media/Coronavirus/Community_Resources/Vaccinations/Print-Materials/Fact-Sheets/Ingredients_English.pdf
To me - there was a rather strong smell with the timing of release of the vaccine for a seasonal virus - was that really just coincidence? Or were they worried they might fail at effectiveness?
It is confounding as well - but one thing viruses do is mess with the immune system - turn it down - they apparently do this with RNA. So if I understand the technology - the spike RNA is packaged in some other viral RNA - instead of producing virions - it only produces this protein - but - to do that - you are causing a novel infection of the machinery of the cell with other RNA bits -(one of the bits viruses mess with has to do with mRNA). I've not found information of what all is encoded on the injected RNA - is it a single strand? I don't think the RNA to code for the spike is the only RNA - don't think it would work otherwise. Likely, they really don't know completely what they are doing - just shooting from the hip.
This is a very dangerous experiment they are doing on the public - looks like the harm is not huge - luck was on their side - I hope there are no long term effects that will show up at 6 mo.
I hope the vaccines are safe and effective enough to end the other madness - I've spent my life reading people's faces - perhaps unconsciously noticing the tiny micro-twitches that people can't blank out. Tuns out we slightly mimic other people's faces - we feel their pain. This ability may not be the same for everyone - perhaps some are happy to block the facial information, but for me, reading faces is about being human, about being alive - it
feels to me that I've been out-of-the-world for a year - like they stole a year of my life.
Reading each others faces is a big part of rubbing up against the world - helps people reality test (not everyone feels the same way at the same time). It is like inflicting psychopathic personalities on everyone - we can't see their face - so we can't feel.
Masking has a history with robbers and surgeons - some surgeons tell me it helps objectify the experience of cutting someone open with a knife. Tribal masks that block face reading has obvious applications in warring peoples.
About the Danish cohort study:
Vaccine efficacy in the first two weeks after vaccination for health care workers was also negative. It was even lower than for nursing house residents.
HC workers - VEadj -1.04
NH residents - VEadj -0.40
Unfortunatelly i've read the study and have no idea what this really means, nor how was it calculated.
Replace 56 with 61 and thats me. Great post Peter to be re-read, and aloud.
Thanks Mat, misread that. It's more logical, HCWs get much more opportunity to meet the virus if exposure needs to be in the low immunity window. NHRs are limited to picking it up at vaccination time or from HCWs I guess.
Gert, many, many infectious/inflammatory processed drop vit D. Covid is one of the few times when supplementing D seems to actually help.
SatFatTW, It is traditional for medical fuckups to blame the patient. What struck me was that perhaps aerosolised covid might be far more ubiquitous that we think and innate immunity keeps most of us safe. Idle speculation on my part.
Peter
Are you seriously suggesting that all of the covid19 cases in India right now are people that have already been vaccinated? Do you have any data at all to support that position?
Phillipa,
Do you have a better explanation?
Peter
The low lymphocytes count picture is from BNT162B1. In BNT162B2 it's less pronounced. I remember it from Dr Vanessa's video after 36 minutes https://youtu.be/xLx2yJAmqdU
Amazing how one's memory improves if your life depends on it. I'll wait until 2023 before deciding to take this concoction.
Awesome post Peter. I wonder if application of biosolids fertilizer could be playing a role too? I'm poor areas of India there are probably a lot of biosolids floating around due to subpar containment/treatment systems in highly dense poor areas.
Phillipa (sorry for the spelling error above),
Actually, eyeballing at the numbers and roll out sequence it looks completely plausible. 52 million 60+ year olds have had the vaccine first dose. There are only 400,000 cases per day now and it was down at around 200,000/day as the elderly were being vaccinated. The problem will be self limiting (it was in the UK) because there are only so many elderly people and once the most at-risk have died they can’t die again. If you were very, very cynical you could even suggest that the marked reduction in serious illness, hospitalisations and fatalities produced once the vaccine has fully worked might simply reflect the immediate post vaccine loss of life making the late post vaccine death rate lower. As I said, you can only die once.
It’s also a conundrum that once you have vaccinated all susceptible people it is impossible to have anyone contract COVID without having already had a vaccine. Then you need very careful studies to see if your vaccine made matters worse in the immediate aftermath of the injection.
Even in the UK we have no information yet about overall numbers of death within 28 days of vaccination or cases within 28 days of vaccination, though the data undoubtedly exist.
Also never forget that India has more than a billion population. Per capita 500,000 cases per day is very low and might even be levelling off, though this might be an artefact of late reporting. Their fatality rate is around one tenth that of the UK. Half of those deaths, and rising, are since they started their massive vaccine roll out. They’ve given 150 million doses already.
Peter
Thanks Ivo, I'll get it corrected when I get the chance.
Justin, hard to say. It's the tie to the vaccine that has my attention
Peter
60% efficacy in 3 mos 60 yrs ago. We came a long way lol
https://www.wsj.com/articles/how-a-more-resilient-america-beat-a-midcentury-pandemic-11619794711
Peter, I figured you hadn't gone down that rabbit hole. Hoping one of your readers has and will weigh in.
altavista, Society has change a lot in our lifetimes. Some aspects for the better, some for the worse. Science is still science but something described as "Science" is now bandied around as a political tool.
I was disgusted at how the Democrats in the USA weaponised covid to attack Trump. I could never be a Trump (he reminds me of Bojo when viewed from 3000 miles away) supporter under any circumstances but watching the setting up of a false narrative to oust him at any cost was appalling. And now they believe their own narrative.
Frightening.
Peter
Two narratives - which one is correct?
The vaccine is mRNA that codes for only the protein spike wrapped in a bit of lipid.
The vaccine is mRNA with other bits added that switch things on and off in the cell like the RNA in a virus?
.. Seems to me that there has to be bits to evade the cells 'surveillance mechanisms' and to tell the cell to excrete the protein once assembled..
,.,
I read that they had a lot of trouble with the lipid capsules - they would trigger immune responses - liver damage - could be what suppresses the immune system?
I suppose it will take a few years before we can possibly have any working knowledge of the unintended consequences.
Yep...
Peter
Peter,
There is quite an uptick in fatalities among 30's and 40's here in India and they have not been vaccinated. The vaccination for 60+ started 1 March and for 45+ started 1 April (ahead of earlier schedule). The 18-45 vaccination was to be started 1 May but there don't seem to be sufficient stock. The slowdown and actual drop in cases for 2 days running perhaps related to slowdown in vaccination?
so here's an anecdote for you
my girlfriend's grandmother is in a care home close to Lyon where all 20 of the residents got both doses of the Pfizer vaccine and 1-2 months later (now) have seen 5 PCR positives of which 3 have covid symptoms.
not great
Gyan, why not? Once granny has had her vaccine and picked up covid at the same time there's no reason why she shouldn't infect the rest of the family, especially those with DMT2. Sort of reverse-shielding.
raphi, that's another whole can of worms. Even before the vaccine trials started it was very clear that there was too much money involved for them to fail, whether the vaccines worked or not. The "yellow arrow" in the UK study diagram in the post will be derived from a population significantly further down the decay curve of the end of the winter resurgence, so should have had a much smaller OR than the pre-vaccine group. I find that disturbing, to say the least.
Peter
« To get ill you still need to meet the virus. You will still look just like a COVID-19 case, who was "probably incubating" at the time of vaccination, or went out partying under lockdown on the day you got your shot. »
Or the virus could have been there all along, properly suppressed to just your enterocytes, and your sudden immunosuppression allows it to surge in the whole body ?
Wash those hands, folks.
The mRNA vaccine reduces “symptoms” of Covid because it downregulates M1 and is anti-inflammatory
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3922422/
This is why I have had patients with “long covid” say they feel better after the vaccine. However, this anti- inflammatory affect comes at the price of immunosuppression- hence the increase in infections.
You may have seen that we are now using inhaled steriods in the treatment of covid - it appears that the mechanism of action is connected to the inverse relationship between Vit D and miR-21.
https://pubmed.ncbi.nlm.nih.gov/31204163/
This is relevant because miR-21 plays a number of pivotal roles in immunometabolism and circadian biology and is involved in most disease conditions.
https://europepmc.org/article/PMC/PMC7953557
You might be particularly interested in it’s role in mitochondrial respiration and cellular lipid content!
https://pubmed.ncbi.nlm.nih.gov/30657727/
As well as diabetes, heart disease and cancer.
Interestingly miR-21 is also connected to circadian control.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0176243
So, why is this relevant to the mRNA vaccine?
Because, it is highly likely miR-21 in involved!
https://crimsonpublishers.com/aics/pdf/AICS.000552.pdf
I suspect they do not realise the potential consequences of an up regulation in miR-21
If Type 2 Diabetes is as undiagnosed in India as it is in the US, yet India still has the second highest level of T2D (behind China), would that not explain some of the rise in infection rates and deaths? India's vaccine rollout just pushed this large vulnerable population over to the infected/serious complication side of the equation.
Here in the US most of the "young" adults who died of Covid looked every bit as a T2D patient, even if they didn't have the "official" diagnosis tagged in their chart.
A possible test of this hypothesis is to see if China slows down their vaccination plans.
Hi Rob,
Well, that last paper was an interesting read. I can't follow the methods in detail but their core finding that microRNAs both suppress allergic reaction to the vaccine (??and the virus) so reduce side effects while enhancing immunity (by interfering with viral replication??) is clearly written with seriously rose tinted spectacles. These people love the Pfizer vaccine(s). I would agree that it would be very plausible that the vaccine might reduce the occasional sniffle or headache that was used to trigger PCR testing in the study which got the virus its emergency authorisation. Fascinating. I couldn't make out how long the effect might last from the paper.
Thanks.
Holly, I Duckducked Sinovacc and it's a traditional inactivated vaccine. It won't have any of the issues of mRNA vaccines but is a dead ringer for ADE, though perhaps not so risky as a live attenuated vaccine...
Peter
E-S, it's becoming pretty clear that the virus is primarily aerosol spread. All that hand gel, social distancing, face nappies. None affect aerosol spread... Opening the windows during a December gale might help!
Peter
Interesting theory about immunosuppression for a while.
As for the summer decrease in covid, this did not happen in the US, depending on where you looked. New England, yes. Texas and other "hot" states, no. To me, this logically makes sense, since covid is "airborne" and everyone in the cooler states was outside, whereas everyone in the hotter states was inside. (Airborne is in quotes because I guess there's a technical definition of this, which the common usage might not fit.)
As for numbers, I've given up trusting these. I think India's death rate is way higher than being reported (you can find many pictures of funeral pyres), but their denominator is also quite large. I also don't think locations like Florida have correct numbers. I mean, when you get rid of a person who had been running your state's covid website because you didn't like the numbers, that's generally not a good thing.
And trying to figure out why something is happening for a disease like this is tough. India, for instance, is a huge country. I look at the US, and even within my small state (CT), mask wearing (as just one example) is all over the map. Most people I know wear them, but where I work, less than half wear them -- at all, ever. I can't analyze outbreaks in my small community, let alone my state, let alone the US or another country (with which I'm not familiar and have never been there).
While I think comorbidities are a detriment, to me, these don't explain everything. I've seen quite a few younger folk who ostensibly were quite healthy get covid and either die or got long covid (or nothing). Like this guy for instance:
https://www.ctinsider.com/local/newstimes/article/He-was-just-wonderful-family-remembers-15195661.php
Lives near me. Seemed to be pretty healthy.
And I see younger folk on Twitter all the time with persistent long-covid systems, and many were athletic beforehand. Dr. Unwin's son, for instance, had POTS for months after covid.
A father my age got covid-19, one of the first ones to get it where I live during the first surge. 12 days on a breathing tube and 50+ days in the hospital. Yet my brother, 2 years younger than me, got it, said it was just like a cold. And I KNOW my brother has comorbidities (smoked for years, overweight, insulin resistant...). A mother who worked where my wife worked and is 7+ years younger than me got covid, recovered, and, in the third (inflammatory) phase, had a massive stroke and died.
To me, comorbidities explain some deaths or susceptibility, but I'm not sure how much. And of course, we have no idea the Vitamin D (or selenium or whatever you think helps) status of any of these people.
I haven't had a flu shot or any other vaccine in decades. But I did get both Pfizer shots. Very few side effects, basically none. I hate to be the lone "pro-vaxxer", but there you have it.
Yes - I believe Vitamin D is the key!
I remember seeing a study that vitamin d levels dropped after a flu jab
and I found this interesting study on BCG vaccination which suggests it increases vit d
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3031626/
There are some reports that this vaccine offers some protection from Covid.
https://www.pnas.org/content/117/30/17720
and it would appear the mRNA vaccine is not the only one that reduces symptoms!
https://www.medindia.net/news/flu-vaccine-decreases-covid-19-symptoms-in-children-199756-1.htm
Peter, I don’t think anyone knows how long the immunosupression will last post vax - it will obviously vary from person - person and I suspect depend upon the time of year!
I am definitely seeing it in practice - followed by more inflammatory conditions like PCR and GCA and even BPV - all of which are linked to low vitamin D levels.
Civiggen - I’m sure you are right about the Deep South - similar issues in India this time of year as heat and humidity increase and also pollution which blocks much of the UVB in the big cities.
One further point - I have been checking Vit d levels of most patients and have noticed surprisingly low levels in lots of young people ( levels in the 20s for people in their 20s is not unusual)
ctviggen, of course we should all make our own choice. I would also just comment that equatorial regions normally have different patterns of influenza seasons cf temperate regions. That would fit with your northern states observation at least. The real outlier to me is South Africa with a peak in their summer.
Peter
Dr. Rob, please deacronymize BPV for me? Thanks.
Benign positional vertigo- I’m seeing a lot of dizziness atm!
https://portlandpress.com/bioscirep/article/39/4/BSR20190142/110877/Serum-levels-of-25-hydroxy-vitamin-D-correlate
Sorry - I also noticed I made a mistake PCR = PMR - polymyalgia rheumatica
Dr. Rob—Thanks! When I first came down with this it was BPPV—guess they've shortened the name. I did not know it was inflammatory or affected by vitamin D. I've managed to mostly train myself out of it (you just tell your vestibules "Deal with it!"), but it crops up very occasionally. This tip could help with for further prevention. And here I thought I was getting plenty of vitamin D…
Yes - you can still call it BPPV and I was also unaware of the connection with Vit D until recently - it’s not something they teach in medical school - in fact, I struggle to find chronic conditions that are not associated with Vit D and now miR-21
@ Dr Rob & Cavenewt, Interesting! I did not know BPPV was such a common ailment. I came down with this 3-weeks ago for the first time (I'm 70 in July). Arriving back home at @ 09:30 I suddenly felt very, very wired. Seemingly, I could not navigate around my flat! Everything was spinning. Eventually, I vomited rather alarmingly and had to lay down on the bathroom floor for about 45 mins. My Vit D levels were seemingly good (I take 1 x 5000 iu per day). Anyway, thanks for the heads-up! It was a very alarming turn of events for me as I'm very rarely ill.
Any reason why this might not be important?
Salk researchers and collaborators show how the protein damages cells, confirming COVID-19 as a primarily vascular disease
Scientists have known for a while that SARS-CoV-2’s distinctive “spike” proteins help the virus infect its host by latching on to healthy cells. Now, a major new study shows that they also play a key role in the disease itself.
The paper, published on April 30, 2021, in Circulation Research, also shows conclusively that COVID-19 is a vascular disease, demonstrating exactly how the SARS-CoV-2 virus damages and attacks the vascular system on a cellular level.
https://www.salk.edu/news-release/the-novel-coronavirus-spike-protein-plays-additional-key-role-in-illness/
Might help explain the negative effects of the vaccine as well as covids preference for those with metabolic syndrome.
Original paper at:
https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
I had the AZ vaccine at the end of March. In early April I experienced vertigo and a shingles rash came up. I have experienced both of these at different times pre-pandemic but the timing of these bouts looks a bit suspicious now. Still battling shingles-brain and exhaustion now.
ctviggen,
Thanks for your comments, it's hard to find places to discuss these things with views from both sides, so nice to see your thoughts. I do wonder if being "athletic" is actually a risk factor, maybe something to do with increased breathing levels, or depressed immune system after exercise, or maybe they're just reported / noticed more often because they seem healthy?
I guess my main reservation with the vaccines is that they are so new, so there should be some trade-off between risk and benefit in the decision to get them, but the authorities seem reluctant to even admit there can be risk. What if there's a rush to produce a new vaccine even more efficiently in the future, 90% of the population get it, and then 50% of them drop dead a couple of years later??? That's obviously really unlikely (I hope), but is it impossible? Shouldn't governments think about this kind of thing?
David, the spike protein is the key because it attacks the ACE2 receptor and drains the cell of energy making you more vulnerable to other infections.
And here lies the rub -
miRNA-21 is needed for the viral replication of influenza A
https://pubmed.ncbi.nlm.nih.gov/29093096/
If a Covid infection or Vaccine increases miRNA-21 - as these studies suggest:
https://crimsonpublishers.com/aics/pdf/AICS.000552.pdf
https://europepmc.org/article/PMC/PMC7844112
https://europepmc.org/article/PMC/PMC7680021
Then people with the spike protein are likely to be more susceptible to severe influenza A infections, with H1N1 being the most likely candidate. Unfortunately, this is the strand which disproportionately affects younger people, due to lack of prior exposure.
My major concern is for babies/infants born during this pandemic, who may have been exposed to the spike protein and have not been exposed to influenza.
https://www.bbc.co.uk/news/world-latin-america-56696907
I suspect this is what we are seeing in Brazil. Children have a mild infection with Covid which makes them more susceptible to influenza
The simple way to decrease deaths would be to ensure Vit D levels are kept high and therefore miRNA-21 low.
Nice pictures in this article from 2013 of the locations in rats where the nanoparticles end up. https://pubmed.ncbi.nlm.nih.gov/23504369/
Thanks Ivo, but the studies it cites are looking at the delivery of siRNAs as disease therapy. They are as protected as possible and are either given IV as they would be for a human, or intraperitoneally if the mouse model is too small for the researchers to get an iv cannula placed. They are not looking to place a very, very nasty antigen on to cell surfaces. The vaccines are given im to get the muscle to be attacked due to expressing foreign protein. Keeping it away from your coronary arteries is a good plan and no one has checked how far the vaccine goes beyond the muscle... The medicines regulators are really balls-ing this one up.
Peter
This might be interesting Peter!
https://www.bloombergquint.com/politics/world-s-most-vaccinated-nation-reintroduces-curbs-as-cases-surge
Seychelles, which has fully vaccinated more of its population against the coronavirus than any other country, has closed schools and canceled sporting activities for two weeks as infections surge. The measures, which include bans on the intermingling of households and the early closure of bars, come even as the country has fully vaccinated more than 60% of its adult population with two doses of C
In the EMA Pfizer assessment report in section 2.3.2. Pharmacokinetics they mention an IV and an IM study.
quote: “ALC-0315 would be eliminated from rat liver in approximately 6-weeks”
and quote “The applicant was asked to discuss the long half-life of ALC-0315 and its effect, discussion on the comparison with patisiran, as well as the impact on the boosts and post treatment contraception duration. The applicant considered that there were no non-clinical safety issues based on the repeat dose toxicity studies at doses (on a mg/kg basis) much greater than administered to humans; this was acceptable to the CHMP.”
It surprises me the regulator just believes what Pfizer says.
https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf
Yes, and Pfizer is the most ethical company on the planet...
Pierre, well yes, most had Sinovac, an inactivated "ordinary" vaccine. If coronavirus vaccines were that easy to make we would have had a cold vaccine decades ago. The mRNA vaccs might actually work, it's quite hard to tell from the published studies. Sinovac appears not to.
Peter
Peter, so where does that leave vector vaccines? They deliver RNA differently, but to the same end, to produce spike proteins. Will they also suppress immunity in the first days? Or maybe not if they act more slowly?
Pfizer hasn't been an ethical company (e.g. pushing statins and then viagra to treat the effects of statins when low dose viagra might have been more beneficial for CVD than statins in the first place), but the BioNtech founders seem to be very ethical people.
Karl, all mRNA vaccines (Pfizer/BioNtech, Moderna and Curevac) use a lipid bubble, so no RNA in the "case".
I am a layperson, not a scientist of any kind, but when they say the spike proteins from the mRNA are mainly expressed in the deltoid muscle tissue, I just have to laugh (in a sardonic, or perhaps increasingly bitter, manner). The mRNA is encased in nanolipids, and nano is extremely small, and therefore able to go places other, larger particles would not be able to.
Also, the thought of anyone's body producing billions (some are saying, it might be trillions) of spike proteins is just revolting on a common, human level (or perhaps even an animal level). If you could tell a dog you wanted to inject it with something that would cause its body to produce billions of tiny spikes, and the dog was capable of understanding you, what do you think its response would be? If the dog was at all sensible, it would bite you and be done with the proposal.
Humans, I'm afraid, at least in the days in which we're living, have much less keen survival instincts than one might have thought. There are predators abroad (and they aren't dogs, or not necessarily...)
Joe, is it better if the real virus makes your cells produce billions of golfballs with spikes?
Maybe it's producing other things that present recognizable patterns that the innate immune system can recognize. Hell, I really don't know. I feel like broadband is potentially better than narrow band here.
We should really be focusing way more research on innate immune function and how to modulate it to become more effective. Vitamin D, low BG, low incorporation in of PUFA into our tissues, etc.
Nicolas Wade in an article yesterday at Medium lays plausible arguments for the lab-created theory of SARS2. Implemented in China, funded by USA. Very interesting and goes to the biochemical nitty-gritty.
@Eric
Several things have to happen - the mRNA I can see getting into the cell as the lipid is absorbed - but then it has to be transported to a ribosome - mostly found in the ER - with only code to produce this protein - some protein would build up in the cell - but then it seems there would be a need to trigger a lytic cycle to release the protein?
Part of being sick with a virus is bursting cells - not just building virion..
I think they must also be building a different protein that causes the lytic cycle? - this varies with different viruses - but the cell either has to burst or have reason to expel the protein through the cell wall - my hunch is they borrowed some genes from some virus to do this - but I don't know. I'm fairly sure that the mitochondria is triggered to cause the lytic cycle. (There are a lot of viruses - with lots of variations).
The mRNA for a protein is usually a loop that keeps getting re-read - but eventually they get degraded. The spike protein would hang around - and get recycled at some point. So I think there is more going on than they have let on to the public (highly controlled message)- but I don't know - likely have part of this wrong.
,.
In the mean time, the CDC has suddenly realized that they are using too many cycles - appears they are seeing 'cases' in people that have been vaccinated. Now they want 28 cycles? might reduce the case numbers by 90%??? Will the public catch on?
People are not quite so stupid as the policy makers assume - the public is now asking why they have to wear masks if the vaccines work. The logic is missing. At some point people notice the 'emperor has no clothes' - and lose trust in the official policy .. Perhaps sanity will return?
Are they telling people to wear masks because Fauci is phobic - or is there something else going on?
Gyan, thanks for that tip. Here's the link
https://nicholaswade.medium.com/origin-of-covid-following-the-clues-6f03564c038
Nicolas Wade has been known for some controversial hypotheses and liberal interpretation of sources, but this appears well laid-out at first glance, and he is fair enough to say it is conjecture. This is really something that looks like it was written for publication in a real paper (i.e. for money) but nobody bit.
So far, only the National Review is reporting (not my favorite news source, but sufficietly serious):
https://www.nationalreview.com/corner/wade-on-the-lab-leak-theory-of-covid/
All this has little bearing on how we should deal with the pandemic now but is interesting still.
Another very good article referenced at the end of the Wade article:
https://yurideigin.medium.com/lab-made-cov2-genealogy-through-the-lens-of-gain-of-function-research-f96dd7413748
Karl, interesting point. I had thought about that, too, whether cells had to burst or be attacked by killer cells to distribute the protein. Surely, that is explained somewhere?
"appears they are seeing 'cases' in people that have been vaccinated".
Does that mean people who have been vaxxed, then get genuinely sick, get tested and found positive? That lines up with what Peter is suggesting here. Or does it mean people who aren't ill but return a positive result therefore in that vague category of 'asymptomatic' which must include all false positives.
The cycles of the PCR test just got changed to 28 by the CDC - “Truth is stranger than fiction, but it is because Fiction is obliged to stick to possibilities; Truth isn't.” ― Mark Twain -
They want the vaccines to look like they are working.
https://www.cdc.gov/vaccines/covid-19/downloads/Information-for-laboratories-COVID-vaccine-breakthrough-case-investigation.pdf
Here is Kansas, I think they were using 35 - 38 - 42 and 45 cycles.. Most often 42..
https://www.communitycareks.org/wp-content/uploads/2020/10/SARS-CoV-2_COVID-19-virus-PCR-Ct-Cutoff-Values100520.pdf
Last summer, the New York Times reported that CTs above 34 almost never detect live virus but most often, dead nucleotides that are not contagious.
I will let someone else run the numbers - but I think there are obviously inflated numbers of cases - and deaths-with-CoVid.
I saw where someone said each cycle doubles the hits - but I don't think it is that simple.
I understand that this hysteria was bonkers - but what I don't understand is the why - I don't think the people in these labs are stupid - how do you get so many people to go along with running 42 cycles?
Not sure how to get people to do a bit of reality testing..
Karl,
Are you the CDC has set the CT for diagnostic purposes? My understanding is they're investigating "breakthrough" cases of COVID - cases in people who have been vaccinated, fully or not. They want to know if the breakthrough is due to a SARS-CoV-2 "variant".
The 28 cycle count is supposed to increase the chance they'll get whole virus for genomic sequencing.
See this Twitter thread.
https://twitter.com/AlexBerenson/status/1387819126270353413
Also https://www.cdc.gov/vaccines/covid-19/downloads/Information-for-laboratories-COVID-vaccine-breakthrough-case-investigation.pdf
India has approved 2-DG as an antiviral drug. Interestingly, per Wikipedia, 2-DG molecule has been proposed as a mimic for ketogenic diet and supposedly shows promise as an anti-epileptic drug.
I am still suffering from the after effects of shingles after my first AZ jab over 1 month ago. Just found out that my nephew, who is fit and in his 20s, also experienced shingles after his first AZ jab (he was vaccinated because he's an 'essential worker'). My nephew was treated with anti-virals by his GP. Seems like a hell of a coincidence if it is an 'extremely rare' side effect.
@Bob
Yes, I know why they are doing it. (In case you didn't know - people have criticized the excessive cycles from the start - some of the canceled content you may have missed?)
Note that "break through cases" is a misleading term - they used it because they didn't want to say "false positives". These tests were never intended to be run at those high cycles. I also think I know why they ran high cycles earlier - to exaggerate the crises - they wanted to scare people into to taking them seriously - virtue signal etc. Running such high cycles is sort of the 'tail waving the dog' - these are the results the policy makers wanted - not reality.
In a sane world, finding fragments rather than actual virus has no use - no utility in defining 'cases'.
Having a few fragments of virus is not the same as being a 'case' - it doesn't even mean you were an 'asymptomatic case' (Someone without fever or symptoms would not be called a 'case' in any other time) - and someone that dies with a few fragments probably died of something else. Creating disinformation is not harmless - it is hurts humanity. So the result of this evil is we don't really know how many real cases there were - we don't know how many real deaths there were. Having clear knowledge of the situation is important to setting sane public health policy.
Here in Kansas, CoVid is pretty much over (for the summer at least - I sort of expect a small bump in the fall) - yet they show about 200 positive 'cases'/day - and about 1 death per day - if they stop the extra cycles on ALL of the testing, the crisis that empowers the officious parrots disappears. What will the new numbers show?
The real puzzle - is Fauci suffering from some sort of phobia? Even for people that are ignorant of the futility of public masking, wearing 2 masks obviously discredits him - makes him look neurotic - a fool. Or, was some other game afoot? There have been only a few voices trying to count the harm caused by these bad policies - over time, I think we will see a drift to a more honest acceptance of the grave cost. - it is as if there were no adults in the room.
Good podcast. I just love Brett and Heather.
https://youtu.be/bU63lsHA0y0
Hi, Karl,
Thanks. Yes, I'm familiar with the PCR cycle threshold controversy. I'm skeptical the purpose was to inflate the case count and scare people. I don't think "they" are that smart. I read recently the purpose was to cast as wide a net as possible to understand the scope of the pandemic. If so, that wide net became entangling when they tested and quarantined asymptomatic people who were positive at high thresholds, which greatly exaggerated the case count. Left hand, right hand, you know how it goes.
Politicians had to react (doing nothing is bad optics). Some used "overreacting" to show how much they could do to "protect us." See Cuomo, Whitmer, Newsom, along with others.
Maybe some day someone will go through all the positive tests and reclassify them using a lower threshold so we get a better idea what really happened or should have happened. Or maybe the records will be "disappeared" so that can't be done.
I'm sure some "breakthrough cases" are false positives, because I don't think the diagnostic CT has changed, but I don't know.
As for Fauci, I agree with those, like Michael Eades, who thinks Fauci is just enjoying his Swan Song in the Sun a little too much. He's a bureaucrat and a politcian before he's a medicine man, and he very capably lies out of both sides of his mouth.
My fond hope is that enough people decline the vaccine that "passports" become economically untenable. The economy needs the "refuseniks" as much as it needs the jabbed.
@ Bob
I don't think you can reclassify the test results after they are run - my understanding is they do the cycles - then test for presence - once. (I could be wrong?)
If they were not trying to scare people to comply - then perhaps it was the money - a powerful motivator. When they could show they had a CoVid case - money flowed. People with repeated negative PCRs were called cases. Public hospitals in particle are always under funding pressure. Did this money help inflate the cycle count? Did the money that flows when they put someone on a ventilator change the standard protocol (at the cost of lives)? Or was the cycle inflation just part of a deception to scare people into following Fauci's misguided advise? Or just part of the political virtue signaling?
So you think it is all about the ego-trip of fame? I guess it could be, but when I saw him wearing two masks at a hearing and say that it was not theater - I sort of believed him - thought he was cracked - of course, I could not see his face - no way to really read his face.. Perhaps I was being a bit gullible? I am staggered at the amount of unmentioned harm that has been done in the name of 'do-gooders' in the last year - it has put a rather large hole in my trust of humanity.
2DG -- Not a new thing, I thought it sounded familiar. From wikip
"2-DG is uptaken by the glucose transporters of the cell. Therefore, cells with higher glucose uptake, for example tumor cells, have also a higher uptake of 2-DG. Since 2-DG hampers cell growth, its use as a tumor therapeutic has been suggested, and in fact, 2-DG is in clinical trials."
A proposed antitumour drug from a while back, touted as a miracle drug for a while. As often happens. IRC there might have been a lawsuit in Germany against someone carelessly administering this drug?? Intravenously?? Perhaps it's not entirely safe...
Looks like it could be the fat burning drug of choice but maybe better to just sidestep the glycolysis by natural means. It will be interesting to see if there is a post covid, post 2-dg intake drop-off in the cancer statistics.
Hmm, the next thing I'd like to see is if any of the therapeutic agents nominated by the people who had developed the cell surface oxygen consumption version of something like the Warburg effect will turn out to have suitable anti-viral properties.
I will search back and find their names and papers!
A couple of NewZealanders et al. Peter blogged about it including links to the papers, and some follow ups:
http://high-fat-nutrition.blogspot.com/2019/01/cell-surface-oxygen-consumption-1.html?m=1
Both 2-DG and metformin demonstrate the “reverse warburg effect” which was hoped to be the Achilles heel of cancer, but never worked out, because for every action there is an equal and opposite reaction.
They also share another property, which I am sure underpins the effect, and would most likely make them anti-viral agents - they down regulate miR-21.
https://pubmed.ncbi.nlm.nih.gov/28230206/
“This study is the first to demonstrate that miR-21 downregulation can sensitise T24 cells to 2-DG, which is one of the most widely investigated pharmacological agents for regulation of glucose metabolism in experimental and clinical oncology”
It is becoming quite apparent, at least to these eyes, that miR-21 is acting as a “redox” energy switch to enable the cell/body to defend against stress/Oxidative stress.
Which is why it is upregulated whenever the ACE2 receptor gets triggered.
For example, hypoxia/HIF-1 leads to an increase in miR-21 which in turn leads to an increase in the mitochondrial protein CYTb (complex 3) of the ETC - I believe it attempts to reduce oxidative stress and ROS by increasing oxygen consumption and ATP to provide the “energy” for the immune system eg NLRP3-inflammasome and even anti-body production by the plasma cells.
This is why it is upregulated in all the chronic diseases, metabolic diseases and cancers.
https://biomarkerres.biomedcentral.com/articles/10.1186/s40364-021-00272-1
It is worth noting that HCQ - the original treatment for Covid - until everything was politicised and corrupted - downregulates miR-21
https://pubmed.ncbi.nlm.nih.gov/24121037/
and also, along with other anti-malarial drugs, inhibits the production of mt cytb.
https://pubs.acs.org/doi/10.1021/acs.jcim.0c01148
There is one further piece to this puzzle - which is the diurnal nature of miR-21 and it’s inverse relationship with Vit D.
miR-21 has been shown to be higher at night and also to be impacted by clock genes ARNTL, BMAL-1 and PER1/2 as well as melatonin.
https://pubmed.ncbi.nlm.nih.gov/31052365/
And, intriguingly - intense blue light.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0176243
So, with miR-21, I believe we are looking at a highly conserved molecule which has allowed an aerobic cell, to deal with the different bioenergetic stresses of day and night environments.
Therefore, I believe Covid and the mRNA vaccine, by up regulating miR-21 will simply put extra stresses upon the cells immunometabolism - and speed up both the aging and pathological processes by increasing entropy in a thermodynamic system.
Pass—"A proposed antitumour drug from a while back, touted as a miracle drug for a while. As often happens. IRC there might have been a lawsuit in Germany against someone carelessly administering this drug?? Intravenously?? Perhaps it's not entirely safe... "
You may be thinking of 3BP, as described by Travis Cristofferson in his book "Tripping Over The Truth", about metabolic treatments for cancer.
Peter, do you have any thoughts on Marek's disease with regards to the covid vaccines? I know Geert Vanden Bossche (nota bene working for the industry) is worried about mass vaccinating during an epidemic and I wonder if it has something to do with this mechanism? Sounds worrisome to me to have a leaky vaccine that only prevents the symptoms of the disease, but not the infection and transmission. Possibly being more dangerous for the unvaccinated, me.
Yes I was!
2dg is related to the compound they use as a marker in PET scanning I think. It still has this property of interfering with glycolysis though.
"CDC Limits Reviews of Vaccinated but Infected, Spurring Concerns"
https://www.bloomberg.com/news/articles/2021-05-09/cdc-limits-reviews-of-vaccinated-but-infected-spurring-concerns?utm_source=facebook&utm_medium=news_tab&utm_content=algorithm
Why?! ... Why would they do this?!
If there were going to be ADE resulting from the vaccines, wouldn't this be the very way to miss it? Or any other problems, really.
The article also provides three anecdotes of breakthrough infections. I noted with dismay that two out of the three experienced symptoms that sound an awful lot like what Peter was musing about in the March 9th post--an autoimmune reaction against skeletal muscle and heart muscle.
"In late March, several days after she began feeling headaches and light-headedness, Melissa Muldoon, a 35-year-old resident of Buffalo, New York, went on a run and lost consciousness.
"Muldoon was taken to an emergency room, where she took a Covid-19 test, she said in an interview. The next day, it came back positive more than a month after she had been fully vaccinated. A week later, she began developing new symptoms, she said, including a loss of smell for certain foods, a racing heart and muscle twitches.
[...]
"'I’m anxious about what happens if there’s no answer,' she said, 'and it just keeps up with random problems or strange things happening with my body that I haven’t experienced before.'"
And this one, too:
"Breana Landon, a 23-year-old Utah resident, has also been experiencing ongoing symptoms.
"Landon tested positive for Covid in late March after being fully vaccinated, she said. It was her second time testing positive. In the first time she was infected last fall, before getting vaccinated, she had respiratory problems that developed into pneumonia. This time, she experienced a whole new set of symptoms, including persisting heart palpitations and pain."
(And the third breakthrough case? - She was a transplant recipient, and her post-vaccination Covid infection was mild. One can't help but think her immunosuppressive drugs prevented any autoimmune reaction against her muscles, while also preventing her from generating enough antibodies to prevent infection.)
Passing out? Racing heart? Muscle twitches? Persisting heart palpitations? Pain?
... Since when are these things typical Covid symptoms?
The article doesn't explicitly say which vaccine these women received, but it calls them "fully vaccinated," suggesting a two-dose regimen, which in the US means an mRNA vaccine.
We need data now as much as ever and the CDC is abandoning us. ... I'm afraid to express my desire to wait-and-see for fear that everyone will lump me in with the tinfoil-hat, microchip-fearing, rewrite-your-DNA crowd. ... Almost everyone I know has been vaccinated. ... I'm so worried.
Re - 2DG - I have been looking for the papers showing the effect of vit-D on this? Can't find them? ( I want to compare the current 'normal' standard to this effect? ( the 30 ng/mL level is really based on preventing rickets - lots of correlative papers about Vit-D, but just about nothing that might show optimal levels (People without shirts in full sun can have levels over 100))
The assumption that 30 is optimal for the other effects of D has no body of controlled studies (There is one intervention study that showed less respiratory infections, but no blood levels were taken). I suspect optimal levels might be over 60. A sane world might fund such research.... )
@Ariadne
They have been misusing the PCR test with excessive cycles - now that they are cutting the cycles back, I think we will see a dramatic change in the number of break-through cases. (What cycle counts were they using in the UK? Did they also change the standard?
The lady in the news story sounds like she was a real case - but vaccine effectiveness is a statistic - not based on a antidote. No vaccine is 100% effective - I don't know what criteria the pharmaceuticals companies were using for a 'case', but I doubt it was the 35 - 38 - 42 - 45 cycles?
Until the CoVid hysteria - viral 'cases' were not defined solely by PCR tests - Other symptoms such as, sudden High fever - respiratory - body aches etc would be needed to say someone was actually sick - thus a 'case'.
The information I'm waiting to see drop is the difference in breakthrough cases with the new lower cycle count - it can provide some numbers to roughly correct the inflated case and death rates they have been pronouncing to the public.
My hunch is the vaccine actually works (similar to influenza vaccines) and is relatively safe - the problems is they have not been honest with the case numbers AND they misrepresented the masking effect - so why should I believe what they are saying now? The level of risk changes who might get a net benefit from a vaccine - without accurate case/death/breakthough numbers, how is it possible to make a rational judgement? I'm not against vaccines, but I do want to have the best risk/benefit numbers - to me it is too soon to know much - and forthright honesty matters.
Karl,
Sorry, I can't find the specifics, but when I was researching D (mainly about 10-12 years ago), it looked like 'ideal' might be 50-60 ng/ml for 'healthy' (metabolically OK individuals) and for those with cancer (maybe other serious challenges as well) 'ideal' was nearer 100.
I have maintained 50-60 and my cancer has been kept in check (zero medication) - obviously purely coincidental, but there you go.
Kevin FST, what type of cancer do you have, if you don't mind me asking? My boss of 13+ years was recently diagnosed with liposarcoma. Started out in is leg and then seems to have spread to his lungs and kidney. With Covid stuff going on, I have been leaning on him to get his d tested and supplement. Fascinating that you have seem to have kept it at bay.
Apparently it can't take part in glycolysis to pyruvate, and accumulates in affected cells only (quite a trick? Peter?). Proponents say it stops viral replication.
Peter could that be because the cell becomes bad at producing energy, like a cancer?
Why is it keto-mimic?
Justin - PCa.
You may have seen it already:
Title: "Informed consent disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease", Timothy Cardozo, Ronald Veazey.
Int J Clin Pract 2021 Mar; 75(3): e13795. doi: 10.1111/ijcp.13795. Epub 2020 Dec 4.
https://pubmed.ncbi.nlm.nih.gov/33113270/
When I read an article in SciAmer last year - my reaction was that the 'bat lady' quotes read like Chinese 'soft' propaganda (a WTF moment - just didn't sound like the words of a bio-nerd). And I didn't buy that she could 'know' it wasn't her virus. And when they closed the lab for 'rectification' and blocked research data - I thought I smelled something rather nasty.
https://www.scientificamerican.com/article/how-chinas-bat-woman-hunted-down-viruses-from-sars-to-the-new-coronavirus1/
This new article provides a good background on what we know today.
https://thebulletin.org/2021/05/the-origin-of-covid-did-people-or-nature-open-pandoras-box-at-wuhan/
I think the original overreaction was because intel agents knew - and were asking virologists and epidemiologist unsettling questions. My take is the likelihood that this came from the lab is over 95%..
It appears that Fauci was THE guy that prevented a hazards review.
Digging into this - it appears that Trump said he thought it came from the lab - when asked for evidence he said “I can’t tell you that. I’m not allowed to tell you that”. So the polarized political world may well have mislead the public - and - I think Fauci most likely had access to the same information. Why wasn't Fauci fired for bypassing safety reviews?
This is not about China - the funding and approval came from the USA.
Gain of function research on viruses is insane.
Well, I sincerely hope this works out.
https://medicalxpress.com/news/2021-05-intranasal-covid-vaccine-candidate-sterilizing.html
I found the same shocking thing than Karl, for two days ago. I had to check with Wall Street journal and nypost... this looks robust. btw, the only point maybe missing is the late start - virus "evolved" perfecly and readily for human epithelium and INSIDE spreading, missed the true flue season as seen 2020?
Fatemperor showed australian newsclips, where Chinese military ponders military use of sars... there is your motivation for gain of function research.
oh boy, there is one remaining possibility ; the borat film was documentary. borat went from Israel to wuhan and sneezed at the market. sure the chinese would endorse that, and WHO would sign on it...
JR
Fast additional comment above; the Pandoras Box defined by Wade and well so, whether the Sars2 escaped from Wuhan lab vs. Natural evolution. Everything points to lab, from codons to animal migration to lab practises. The remaining possibility, straight leap bat-to-human, would require that bats get sars2. They don't.
Late start early 2020 vs. Fall spreading 2020... the engineered to infect -virus missed a few trains 2019?
JR
Looks like Israel might start to question their vaccine data. Wonder how long it will take to finally publish something......
"The Israel Health Ministry is examining a small number of cases related to inflammation of the heart muscle called ‘myocarditis’ in individuals inoculated with Pfizer and BioNtech’s Covid-19 vaccine."
"Ash added: “The Health Ministry is currently examining whether there is an excess in morbidity and whether it can be attributed to the vaccines.”
"So far, the ministry has not arrived at any conclusions."
https://www.pharmaceutical-technology.com/news/israel-myocarditis-pfizer-vaccine/?fbclid=IwAR2NJgoAVfqD1Prf4mjt5HHSZv4j0D0fSz62W4oI5NkAFxdu9mhdfO-J3SU
Apparently a big slug of CDC, FDA, and NIAID employees are anti-science. Or they've been reading Hyperlipid.
https://twitter.com/kerpen/status/1393022731373973504
Peter, have you seen any increase in cortisol levels or Cushing syndrome in dogs recently?
https://www.springermedizin.de/covid-19/pneumonie/the-effect-of-omega-3-fatty-acid-supplementation-on-clinical-and/19016640
Googling "corona pufa" finds a whole slew of these. Arrgh.
Anecdotal, but a day after having the second Pfizer vaccine my lymphocyte count was 0.8 and neutrophils were >6. My normal values for these are ~1.5 and 1.5-3 respectively.
Thoughts? https://www.liebertpub.com/doi/full/10.1089/vim.2020.0330?fbclid=IwAR0Y9rvW4We4XUR0PQIgozScroxNX6x6kB7HjPCzsK5e1D0RKVxwIkHaS4Q
More aaargh:
German risk assessment agency warns against taking vit D:
https://www.bfr.bund.de/cm/343/vitamin-d-das-immunsystem-und-covid-19.pdf
Study shows that vit D sufficiency does not protect against infection with Covid once health and socioeconomic status are taken into account:
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2779952?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=051921
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2779959
This is really rich! Prof. Raoult of U Marseille has been going after Dr. Elisabeth Bik who first called out problems with his hydroxychloroquine study by insulting her on national television and social media. Now he has filed a lawsuit against her and the administrator of PUBPEER and posted her home address and financial information online.
https://www.theguardian.com/science/2021/may/22/world-expert-in-scientific-misconduct-faces-legal-action-for-challenging-integrity-of-hydroxychloroquine-study
From today's guardian newsfeed. Apparently, the two vector vaccines send spike protein into the nucleus (why?), where it gets spliced, expelled and can wreak havoc in the bloodstream.
The preprint is here:
https://www.researchsquare.com/article/rs-558954/v1
Guardian arcticle:
Scientists in Germany claim to have solved the cause of the rare blood clotting events linked to the Oxford/AstraZeneca and Johnson & Johnson vaccines and believe the jabs could be fixed to prevent the reaction altogether, the FT (paywall) reports.
Rolf Marschalek, a professor at Goethe university in Frankfurt who has been leading research into the rare condition since March, said his research showed that the problem lies with the adenovirus vectors that both vaccines use to deliver the spike protein of the virus into the body.
In a preprint paper published today, the scientists wrote that the delivery mechanism means the vaccines send the spike protein into the cell nucleus as opposed to the cytosol fluid found inside the cell where the virus normally produces proteins.
According to Marschalek’s research, once inside the cell nucleus, certain parts of the spike protein splice, creating mutant versions, which are unable to bind to the cell membrane where important immunisation takes place; instead, the floating mutant proteins are secreted by cells into the body, which is what triggers blood clots in roughly one in 100,000 people.
In contrast, with mRNA-based vaccines, such as the BioNTech/Pfizer and Moderna jabs, the spike’s genetic material is delivered to the cell fluid and it never enters the nucleus. Marschalek told the FT that when virus genes are in the nucleus they can create “some problems”.
He believes there is a “way out” if the vaccine developers can adapt the sequence of the spike protein to prevent splicing.
You can read the FT’s exclusive story here.
Maybe we should have a clinical trial before approval?
Peter
"Maybe we should have a clinical trial before approval?"
Peter, like you, I took some computer programming in college. Unlike you, I ended my career as a software developer. Along the way, I saw some "cowboys" in action "fixing" important bugs and getting them to the client ASAP.
The manager finally laid down the law. "No more five-minute bug fixes!"
Amen Bob!
Perhaps this is safer, in the short term anyway:
https://biotechdispatch.com.au/news/testing-shows-starpharmas-viraleze-highly-active-against-uk-covi
Bit late for us in the UK Pass. Currently the seven day rolling average is 6 deaths per day and there are less patients hospitalised for COVID-19 than there are hospitals. Prison for SAGE would be nice. Whitty and Valance might be better sectioned under the mental health act. In Broadmoor.
Peter
Our federal pollies are probably better advised than yours, or less conflictedly, but they're still cut from the same cloth as yer Boris. They aren't so clever at being obtuse though and I think they look up to BJ with awe.
It's sickening.
The people who do the heavy lifting here are the individual state government leaders and their advisers. The States are semi- autonomous and locally responsive.
fyi: scary stuff for non-elderly females getting the shot
Japanese bio-distribution study:
https://click.convertkit-mail.com/mvu972x0gnt5h6np6lsm/08hwh9hm7vd9rlal/aHR0cHM6Ly93d3cucG1kYS5nby5qcC9kcnVncy8yMDIxL1AyMDIxMDIxMjAwMS82NzIyMTIwMDBfMzAzMDBBTVgwMDIzMV9JMTAwXzEucGRm
When these vaccines were developed the idea was that the lipid nanoparticles (LNP) carrying the mRNA template would be taken into the muscle cells, travel to the ribosomes (the intracellular protein synthesis factories), and produce the spike proteins. These would be released from the cells and trip the immune response, which would then provide protection against SARS2. Although many people wondered whether the LNP would stay put in the muscle cells or would end up in other places. As you can see, the LNP do not stay localized in the shoulder muscles. They move about. They can be found in both whole blood and plasma peaking at a couple of hours and gradually dropping off over 48 hours. Levels continue to accumulate in slowly growing numbers in bone marrow and in rapidly increasing numbers in the ovaries.
Yes, and there are moves afoot to force vaccinate children for school un the UK.
There is no end to this
Peter
forgot to credit Dr. M Eades for the above and this link
https://www.bitchute.com/video/wUlpFlXb3KSz/
Post a Comment